Pediatric Urology Research Enterprise, Department of Pediatric Urology, Division of Urology, Department of Surgery, Children's Hospital Colorado, University of Colorado Denver Anschutz Medical Campus, 13123 East 16th Avenue, Mailbox B-463, Aurora, CO, 80045, USA.
Adult and Child Center for Health Outcomes Research and Delivery Science, University of Colorado Denver Anschutz Medical Campus, Aurora, CO, USA.
Int Urol Nephrol. 2021 Aug;53(8):1485-1495. doi: 10.1007/s11255-021-02866-y. Epub 2021 May 4.
Studies based on administrative databases show that infant pyeloplasty is associated with minority race/ethnicity but lack clinical data that may influence treatment. Our objective was to identify clinical and demographic factors associated with pyeloplasty in infants from three large tertiary centers.
We reviewed infants with unilateral Society for Fetal Urology (SFU) grade 3-4 hydronephrosis seen at three tertiary centers from 2/1/2018 to 9/30/2019. Patients were excluded if > 6 months old or treated surgically prior to the initial visit. Outcomes were: pyeloplasty < age 1 year and SFU grade on most recent ultrasound (US) within the first year. Covariables included: age at the initial visit, race/ethnicity, treating site, insurance type, febrile UTI, and initial imaging findings. Univariable and multivariable analyses were performed using log-rank tests and Cox proportional hazards models, respectively.
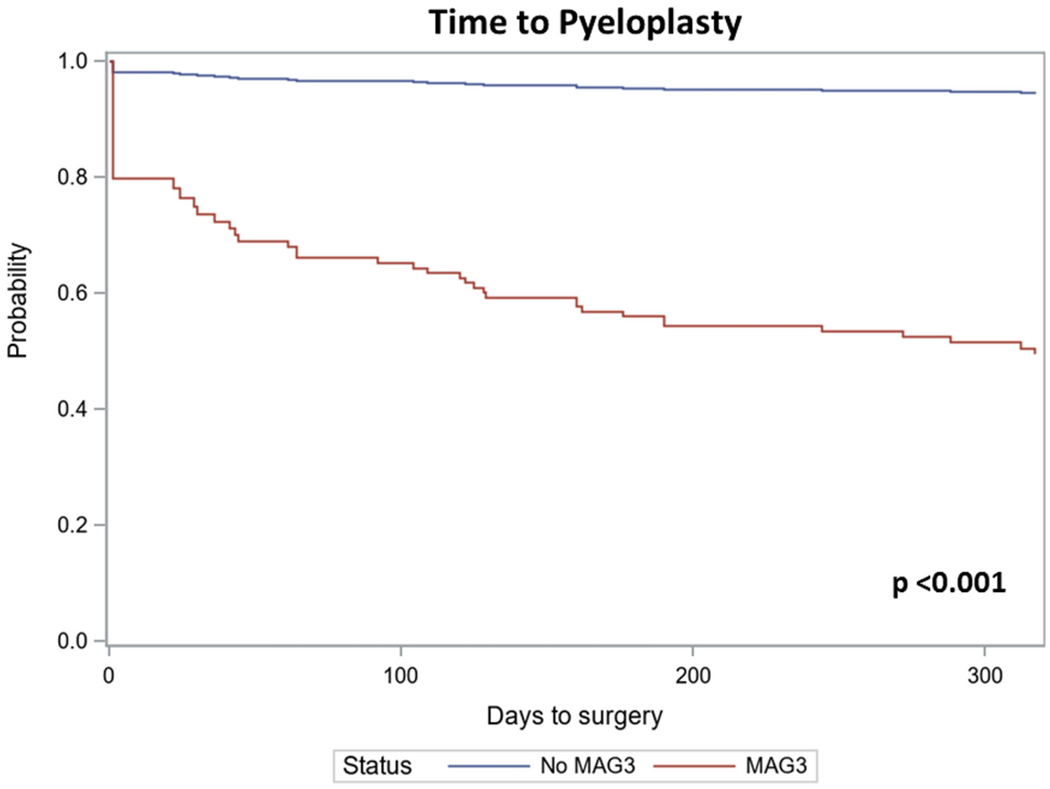
197 patients met study criteria; 19.3% underwent pyeloplasty. Pyeloplasty was associated with: treating site (p = 0.03), SFU 4 on initial US (p = 0.001), MAG-3 (p < 0.001), and T½ > 20 min (p < 0.001) in patients undergoing a MAG-3 (n = 107). MAG-3 (p < 0.001) and location (p = 0.08) were associated with earlier time to pyeloplasty on multivariable Cox analysis. In infants with follow-up US (n = 115), initial SFU grade, MAG-3 evaluation or findings, and pyeloplasty were not associated with improvement of hydronephrosis.
We found that infant pyeloplasty rates vary between sites. Prolonged T½ was associated with surgery despite prior studies suggesting this is a poor predictor of worsening dilation or function. These findings suggest the need to standardize evaluation and indications for intervention in infants with suspected UPJ obstruction.
基于行政数据库的研究表明,婴儿肾盂成形术与少数民族种族/族裔有关,但缺乏可能影响治疗的临床数据。我们的目的是确定与三家大型三级中心的婴儿肾盂成形术相关的临床和人口统计学因素。
我们回顾了 2018 年 2 月 1 日至 2019 年 9 月 30 日期间在三家三级中心就诊的单侧胎儿泌尿外科学会(SFU)3-4 级肾盂积水的婴儿。如果患者年龄大于 6 个月或在首次就诊前已接受手术治疗,则将其排除在外。结果是:肾盂成形术<1 岁,且首次就诊后 1 年内的最新超声(US)SFU 分级。协变量包括:首次就诊时的年龄、种族/族裔、治疗部位、保险类型、发热性尿路感染和初始影像学发现。使用对数秩检验和 Cox 比例风险模型分别进行单变量和多变量分析。
197 名患者符合研究标准;19.3%接受了肾盂成形术。肾盂成形术与:治疗部位(p=0.03)、初始 US 的 SFU 4 级(p=0.001)、MAG-3(p<0.001)和 T½>20 分钟(p<0.001)有关,这些患者接受了 MAG-3(n=107)。多变量 Cox 分析显示,MAG-3(p<0.001)和位置(p=0.08)与肾盂成形术的较早时间相关。在有随访 US(n=115)的婴儿中,初始 SFU 分级、MAG-3 评估或结果以及肾盂成形术与肾积水的改善均无关。
我们发现,婴儿肾盂成形术的比例在不同的部位之间有所不同。尽管先前的研究表明 T½ 延长是病情恶化或功能恶化的不良预测指标,但 T½ 延长与手术相关。这些发现表明需要在疑似 UPJ 梗阻的婴儿中标准化评估和干预的适应证。