Sehgal Kanika, Fadel Hind J, Tande Aaron J, Pardi Darrell S, Khanna Sahil
Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN, USA.
Division of Infectious Diseases, Mayo Clinic, Rochester, MN, USA.
Infect Drug Resist. 2021 Apr 28;14:1645-1648. doi: 10.2147/IDR.S305349. eCollection 2021.
Coronavirus infectious disease 2019 (COVID-19) is primarily a respiratory disease. However, it may manifest with gastrointestinal symptoms that may overlap with infection (CDI). COVID-19 appears to have higher mortality in those with comorbidities. We aimed to assess the outcomes of coinfection in these patients.
A retrospective chart review was conducted to identify patients with CDI and COVID-19 from January 1st, 2020 to November 17th, 2020. Both infections were diagnosed via PCR. Clinical features, treatment for COVID-19 and CDI and outcomes including intensive care unit admission, colectomy, 30 day-mortality and long-term complications were analyzed.
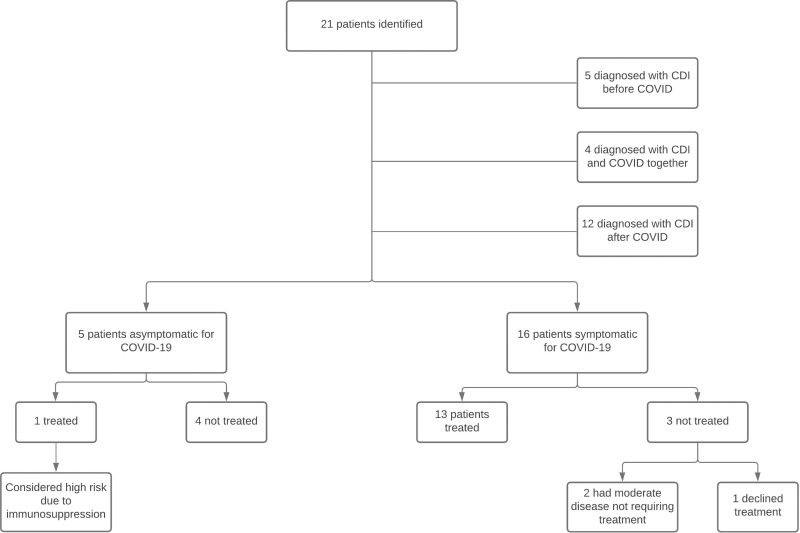
Overall, 21 patients (20 hospitalized) with median age 70.9 years (range 51.8-90.7 years) had CDI and COVID-19 within 4 weeks of each other. Of these, 4 patients (19%) with CDI were diagnosed with COVID-19 at the time of admission, 12 (57%) had CDI diagnosed after COVID-19, and 5 (23.9%) developed COVID-19 within 4 weeks after CDI. Fourteen patients (66.7%) were treated with medications directed against COVID-19 including remdesivir and dexamethasone (n=7), remdesivir with convalescent plasma (n= 1), remdesivir (n= 5) and dexamethasone (n=1). The most common treatment for CDI was oral vancomycin in 20 patients (95.2%), and 1 patient received intravenous metronidazole. No patient required colectomy for CDI but 2 (9.5%) required ICU admission. Four patients (19%) died likely due to COVID-19 with median age 80 years (range 61-90 years).
The relationship between COVID-19 and CDI is poorly understood, and studies are required to further investigate this association. Whether coinfection results in a worsening of outcomes, including mortality and clinical course, are questions that should be answered in future research studies. Diagnosing both infections for appropriate management is vital in light of overlapping symptoms.
2019冠状病毒病(COVID-19)主要是一种呼吸道疾病。然而,它可能表现出与艰难梭菌感染(CDI)重叠的胃肠道症状。COVID-19在合并症患者中似乎具有更高的死亡率。我们旨在评估这些患者合并感染的结局。
进行了一项回顾性病历审查,以识别2020年1月1日至2020年11月17日期间患有CDI和COVID-19的患者。两种感染均通过聚合酶链反应(PCR)诊断。分析了临床特征、COVID-19和CDI的治疗以及包括重症监护病房入院、结肠切除术、30天死亡率和长期并发症在内的结局。
总体而言,21例患者(20例住院),中位年龄70.9岁(范围51.8 - 90.7岁),在彼此4周内患有CDI和COVID-19。其中,4例(19%)患有CDI的患者在入院时被诊断出患有COVID-19,12例(57%)在COVID-19后被诊断出患有CDI,5例(23.9%)在CDI后4周内出现COVID-19。14例患者(66.7%)接受了针对COVID-19的药物治疗,包括瑞德西韦和地塞米松(n = 7)、瑞德西韦与恢复期血浆(n = 1)、瑞德西韦(n = 5)和地塞米松(n = 1)。CDI最常见的治疗方法是20例患者(95.2%)口服万古霉素,1例患者接受静脉注射甲硝唑。没有患者因CDI需要进行结肠切除术,但2例(9.5%)需要入住重症监护病房。4例患者(19%)可能因COVID-19死亡,中位年龄80岁(范围61 - 90岁)。
对COVID-19与CDI之间的关系了解甚少,需要进行研究以进一步调查这种关联。合并感染是否会导致包括死亡率和临床病程在内的结局恶化,是未来研究中应回答的问题。鉴于症状重叠,对两种感染进行诊断以进行适当管理至关重要。