Department of Cardiovascular Medicine, Sixth Medical Center, Chinese PLA General Hospital, Beijing, China.
Department of Cardiology, Second Medical Center, Chinese PLA General Hospital, Beijing, China.
Oxid Med Cell Longev. 2021 Apr 12;2021:6663948. doi: 10.1155/2021/6663948. eCollection 2021.
To explore the association between EAT volume and plaque precise composition and high risk plaque detected by coronary computed tomography angiography (CCTA).
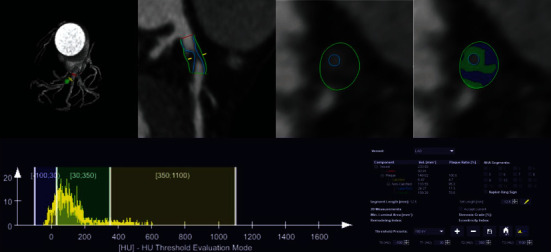
101 patients with suspected coronary artery disease (CAD) underwent CCTA examination from March to July 2019 were enrolled, including 70 cases acute coronary syndrome (ACS) and 31 cases stable angina pectoris (SAP). Based on CCTA image, atherosclerotic plaque precise compositions were analyzed using dedicated quantitative software. High risk plaque was defined as plaque with more than 2 high risk features (spotty calcium, positive remolding, low attenuation plaque, napkin-ring sign) on CCTA image. The association between EAT volume and plaque composition was assessed as well as the different of correlation between ACS and SAP was analyzed. Multivariable logistic regression analysis was used to explore whether EAT volume was independent risk factors of high risk plaque (HRP).
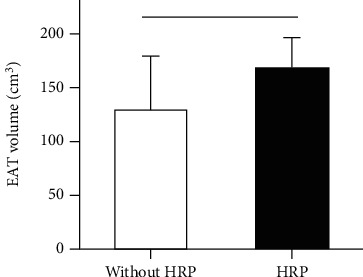
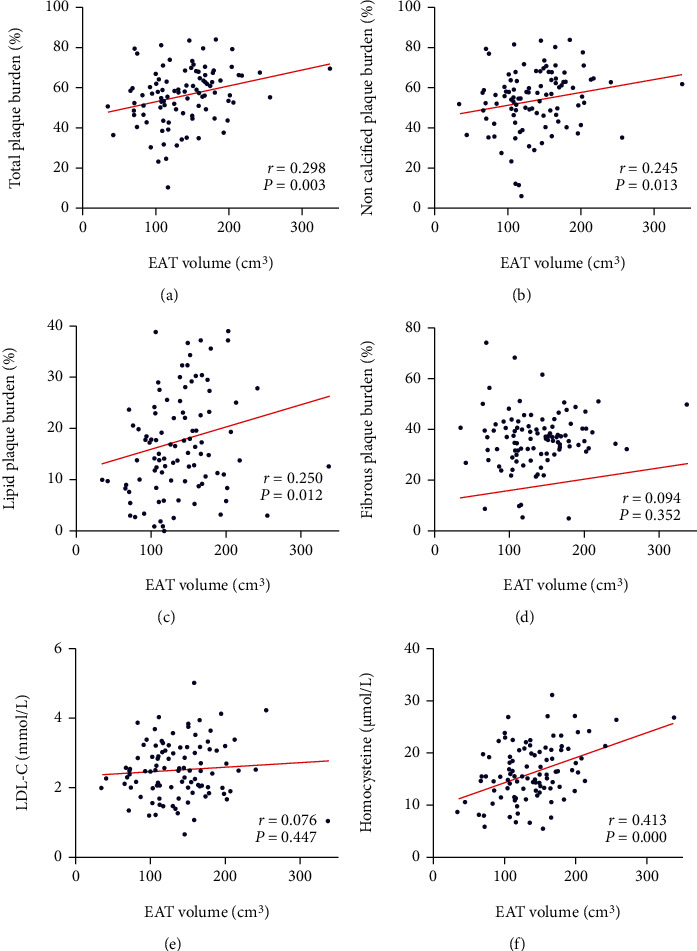
EAT volume in the ACS group was significantly higher than that of the SAP group (143.7 ± 49.8 cm vs. 123.3 ± 39.2 cm, = 0.046). EAT volume demonstrated a significant positive correlation with total plaque burden ( = 0.298, = 0.003), noncalcified plaque burden ( = 0.245, = 0.013), lipid plaque burden ( = 0.250, = 0.012), and homocysteine ( = 0.413, ≤ 0.001). In ACS, EAT volume was positively correlated with total plaque burden ( = 0.309, = 0.009), noncalcified plaque burden ( = 0.242, = 0.044), and lipid plaque burden ( = 0.240, = 0.045); however, no correlation was observed in SAP. Patients with HRP have larger EAT volume than those without HRP (169 ± 6.2 cm vs. 130.6 ± 5.3 cm, = 0.002). After adjustment by traditional risk factors and coronary artery calcium score (CACS), EAT volume was an independent risk predictor of presence of HRP (OR: 1.018 (95% CI: 1.006-1.030), = 0.004).
With the increasing EAT volume, more dangerous plaque composition burdens increase significantly. EAT volume is a risk predictor of HRP independent of convention cardiovascular risk factors and CACS, which supports the potential impact of EAT on progression of coronary atherosclerotic plaque.
探讨 EAT 体积与冠状动脉计算机断层扫描血管造影(CCTA)检测到的斑块精确成分和高危斑块之间的关系。
2019 年 3 月至 7 月,纳入 101 例疑似冠心病(CAD)患者行 CCTA 检查,包括 70 例急性冠状动脉综合征(ACS)和 31 例稳定性心绞痛(SAP)患者。基于 CCTA 图像,使用专用定量软件分析动脉粥样硬化斑块的精确成分。定义高危斑块为 CCTA 图像上具有超过 2 个高危特征(点状钙、阳性重塑、低衰减斑块、餐巾环征)的斑块。评估 EAT 体积与斑块成分之间的关系,并分析 ACS 和 SAP 之间相关性的差异。多变量逻辑回归分析用于探讨 EAT 体积是否为高危斑块(HRP)的独立危险因素。
ACS 组的 EAT 体积明显高于 SAP 组(143.7±49.8cm 比 123.3±39.2cm, = 0.046)。EAT 体积与总斑块负荷呈显著正相关( = 0.298, = 0.003)、非钙化斑块负荷( = 0.245, = 0.013)、脂质斑块负荷( = 0.250, = 0.012)和同型半胱氨酸( = 0.413, ≤ 0.001)。在 ACS 中,EAT 体积与总斑块负荷( = 0.309, = 0.009)、非钙化斑块负荷( = 0.242, = 0.044)和脂质斑块负荷( = 0.240, = 0.045)呈正相关;然而,在 SAP 中则无相关性。HRP 患者的 EAT 体积明显大于无 HRP 患者(169±6.2cm 比 130.6±5.3cm, = 0.002)。在调整传统危险因素和冠状动脉钙评分(CACS)后,EAT 体积是 HRP 存在的独立危险因素(OR:1.018(95%CI:1.006-1.030), = 0.004)。
随着 EAT 体积的增加,危险性斑块成分负担明显增加。EAT 体积是独立于传统心血管危险因素和 CACS 的 HRP 预测因子,这支持 EAT 对冠状动脉粥样硬化斑块进展的潜在影响。