IHU LIRYC-CHU Bordeaux, Univ. Bordeaux, Inserm U1045, Avenue du Haut Lévêque, 33604 Pessac, France.
Department of Cardiovascular Imaging, Hôpital Cardiologique du Haut-Lévêque, CHU de Bordeaux, Avenue de Magellan, 33604 Pessac, France.
Europace. 2021 Sep 8;23(9):1391-1399. doi: 10.1093/europace/euab090.
Extra-atrial injury can cause complications after catheter ablation for atrial fibrillation (AF). Pulsed field ablation (PFA) has generated preclinical data suggesting that it selectively targets the myocardium. We sought to characterize extra-atrial injuries after pulmonary vein isolation (PVI) between PFA and thermal ablation methods.
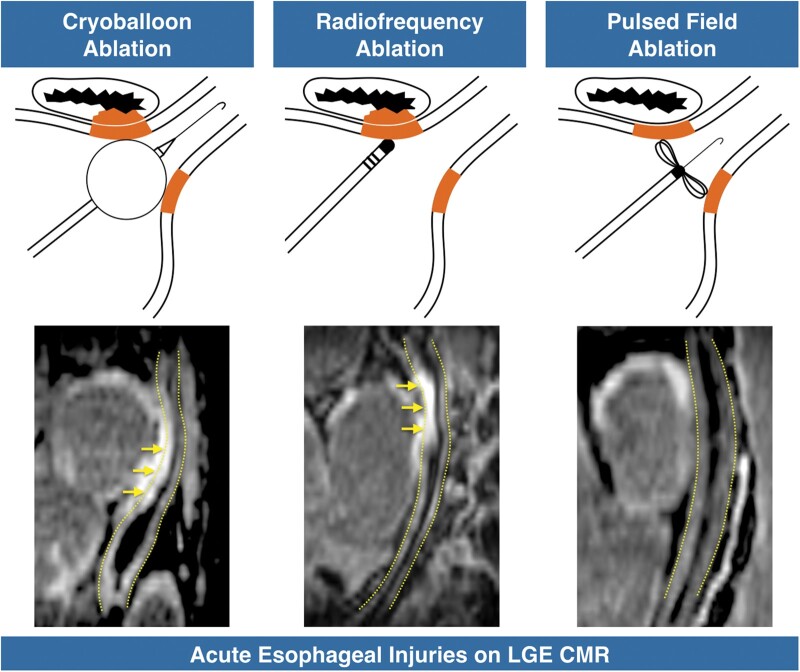
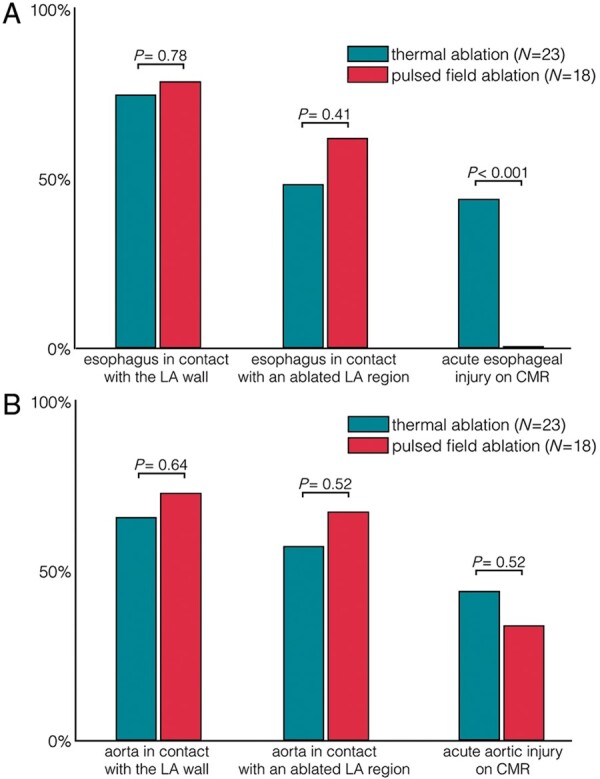
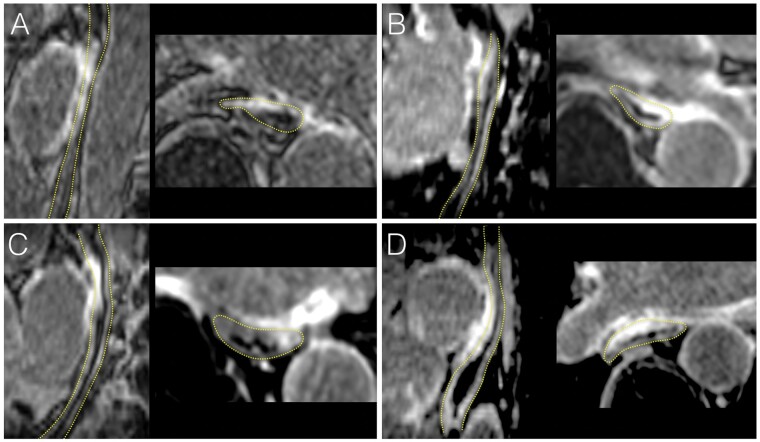
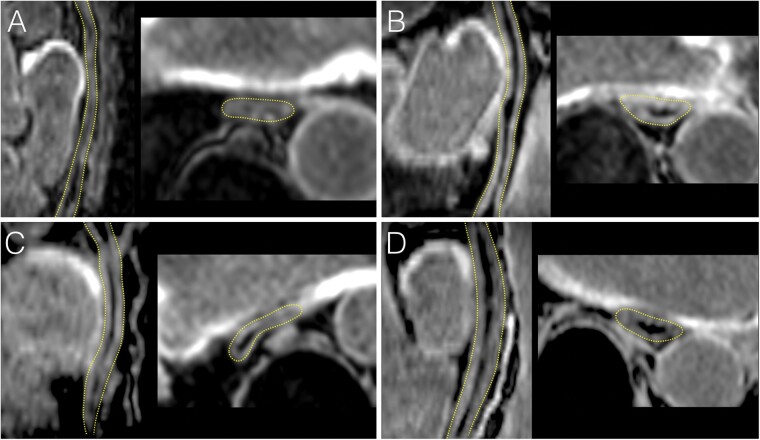
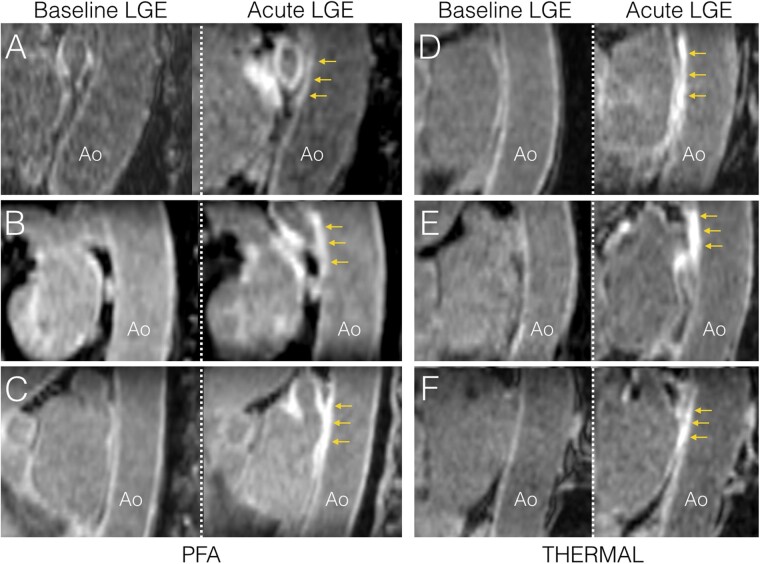
Cardiac magnetic resonance (CMR) imaging was performed before, acutely (<3 h) and 3 months post-ablation in 41 paroxysmal AF patients undergoing PVI with PFA (N = 18, Farapulse) or thermal methods (N = 23, 16 radiofrequency, 7 cryoballoon). Oesophageal and aortic injuries were assessed by using late gadolinium-enhanced (LGE) imaging. Phrenic nerve injuries were assessed from diaphragmatic motion on intra-procedural fluoroscopy. Baseline CMR showed no abnormality on the oesophagus or aorta. During ablation procedures, no patient showed phrenic palsy. Acutely, thermal methods induced high rates of oesophageal lesions (43%), all observed in patients showing direct contact between the oesophagus and the ablation sites. In contrast, oesophageal lesions were observed in no patient ablated with PFA (0%, P < 0.001 vs. thermal methods), despite similar rates of direct contact between the oesophagus and the ablation sites (P = 0.41). Acute lesions were detected on CMR on the descending aorta in 10/23 (43%) after thermal ablation, and in 6/18 (33%) after PFA (P = 0.52). CMR at 3 months showed a complete resolution of oesophageal and aortic LGE in all patients. No patient showed clinical complications.
PFA does not induce any signs of oesophageal injury on CMR after PVI. Due to its tissue selectivity, PFA may improve safety for catheter ablation of AF.
心房颤动(房颤)导管消融术后的心房外损伤可导致并发症。脉冲场消融(PFA)已产生临床前数据,表明其选择性靶向心肌。我们旨在描述 PFA 和热消融方法进行肺静脉隔离(PVI)后心房外损伤。
41 例阵发性房颤患者行 PVI,其中 18 例(Farapulse)采用 PFA,23 例采用热消融方法(16 例射频,7 例冷冻球囊)。在消融前、术后 3 小时内(<3 小时)和 3 个月时,进行心脏磁共振(CMR)成像,评估食管和主动脉损伤。通过延迟钆增强(LGE)成像评估膈神经损伤。术中透视评估膈神经运动。CMR 基线显示食管或主动脉无异常。在消融过程中,无患者出现膈神经麻痹。热消融方法导致食管损伤发生率较高(43%),所有患者均观察到食管与消融部位直接接触。相比之下,采用 PFA 消融的患者无一例出现食管损伤(0%,P<0.001 与热消融方法相比),尽管食管与消融部位的直接接触率相似(P=0.41)。热消融后 23 例患者中有 10 例(43%)在下行主动脉上检测到急性损伤,18 例患者中有 6 例(33%)采用 PFA (P=0.52)。3 个月时 CMR 显示所有患者食管和主动脉 LGE 完全消退。无患者出现临床并发症。
PFA 不会导致 PVI 后 CMR 显示食管损伤的任何迹象。由于其组织选择性,PFA 可能会提高房颤导管消融的安全性。