Ahmanson Translational Theranostics Division, Department of Molecular & Medical Pharmacology, David Geffen School of Medicine, University of California, Peter Norton Medical Building, 200 Medical Plaza, Suite B-114-51, Los Angeles, CA, 90095-7370, USA.
Jonsson Comprehensive Cancer Center, University of California Los Angeles, Los Angeles, CA, USA.
BMC Cancer. 2021 May 7;21(1):512. doi: 10.1186/s12885-021-08026-w.
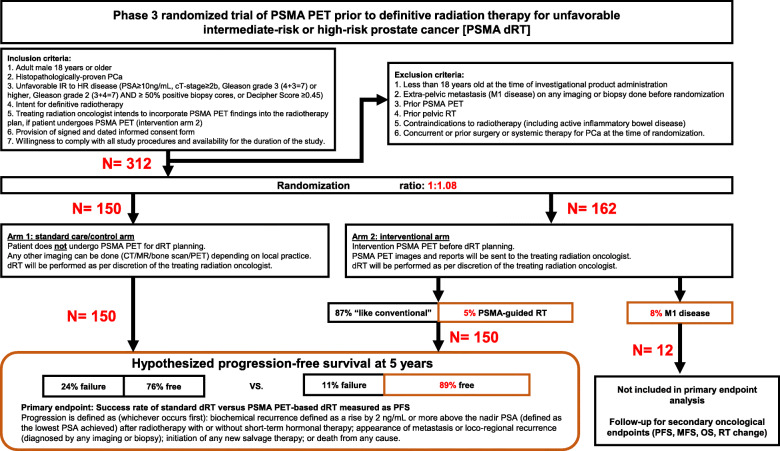
Definitive radiation therapy (dRT) is an effective initial treatment of intermediate-risk (IR) and high-risk (HR) prostate cancer (PCa). PSMA PET/CT is superior to standard of care imaging (CT, MRI, bone scan) for detecting regional and distant metastatic PCa. PSMA PET/CT thus has the potential to guide patient selection and the planning for dRT and improve patient outcomes.
This is a multicenter randomized phase 3 trial (NCT04457245). We will randomize 312 patients to proceed with standard dRT (control Arm, n = 150), or undergo a PSMA PET/CT scan at the study site (both 18F-DCFPyL and 68Ga-PSMA-11 can be used) prior to dRT planning (intervention arm, n = 162). dRT will be performed at the treating radiation oncologist facility. In the control arm, dRT will be performed as routinely planned. In the intervention arm, the treating radiation oncologist can incorporate PSMA PET/CT findings into the RT planning. Androgen deprivation therapy (ADT) is administered per discretion of the treating radiation oncologist and may be modified as a result of the PSMA PET/CT results. We assume that approximately 8% of subjects randomized to the PSMA PET arm will be found to have M1 disease and thus will be more appropriate candidates for long-term systemic or multimodal therapy, rather than curative intent dRT. PET M1 patients will thus not be included in the primary endpoint analysis. The primary endpoint is the success rate of patients with unfavorable IR and HR PCa after standard dRT versus PSMA PET-based dRT. Secondary Endpoints (whole cohort) include progression free survival (PFS), metastasis-free survival after initiation of RT, overall survival (OS), % of change in initial treatment intent and Safety.
This is the first randomized phase 3 prospective trial designed to determine whether PSMA PET/CT molecular imaging can improve outcomes in patients with PCa who receive dRT. In this trial the incorporation of PSMA PET/CT may improve the success rate of curative intent radiotherapy in two ways: to optimize patient selection as a biomarker and to personalizes the radiotherapy plan.
UCLA IND#147591 ○ Submission: 02.27.2020 ○ Safe-to-proceed letter issued by FDA: 04.01.2020 UCLA IRB #20-000378 ClinicalTrials.gov Identifier NCT04457245 . Date of Registry: 07.07.2020. Essen EudraCT 2020-003526-23.
确定性放射治疗(dRT)是中危(IR)和高危(HR)前列腺癌(PCa)的有效初始治疗方法。PSMA PET/CT 比标准护理成像(CT、MRI、骨扫描)更能检测局部和远处转移性 PCa。因此,PSMA PET/CT 有可能指导患者选择和 dRT 规划,并改善患者预后。
这是一项多中心随机 3 期试验(NCT04457245)。我们将随机分配 312 名患者接受标准 dRT(对照组,n=150)或在 dRT 计划前在研究地点进行 PSMA PET/CT 扫描(18F-DCFPyL 和 68Ga-PSMA-11 均可使用)(干预组,n=162)。dRT 将在治疗放射肿瘤学家的机构进行。在对照组中,dRT 将按常规计划进行。在干预组中,治疗放射肿瘤学家可以将 PSMA PET/CT 结果纳入 RT 计划中。去势治疗(ADT)将由治疗放射肿瘤学家决定,并可能因 PSMA PET/CT 结果而改变。我们假设随机分配到 PSMA PET 组的大约 8%的患者将被发现患有 M1 疾病,因此更适合接受长期系统或多模式治疗,而不是治愈性意图的 dRT。因此,PET M1 患者将不包括在主要终点分析中。主要终点是标准 dRT 后 IR 和 HR PCa 患者的治疗成功率与 PSMA PET 为基础的 dRT 相比。次要终点(全队列)包括无进展生存期(PFS)、RT 开始后的无转移生存期、总生存期(OS)、初始治疗意图变化百分比和安全性。
这是第一项旨在确定 PSMA PET/CT 分子成像是否可以改善接受 dRT 的 PCa 患者结局的前瞻性 3 期随机试验。在这项试验中,PSMA PET/CT 的纳入可以通过两种方式提高有治愈意图的放疗的成功率:通过生物标志物优化患者选择和个性化放疗计划。
加州大学洛杉矶分校 IND#147591 ○提交日期:02.27.2020 ○FDA 发出安全进行信函:04.01.2020 加州大学洛杉矶分校 IRB #20-000378 ClinicalTrials.gov 标识符 NCT04457245。注册日期:07.07.2020。Essen EudraCT 2020-003526-23。