Adams Phillip S, Corcoran Timothy E, Lin Jiuann-Huey, Weiner Daniel J, Sanchez-de-Toledo Joan, Lo Cecilia W
Division of Pediatric Anesthesiology, Department of Anesthesiology and Perioperative Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States.
Division of Critical Care Medicine, Department of Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States.
Front Cardiovasc Med. 2021 Apr 23;8:652158. doi: 10.3389/fcvm.2021.652158. eCollection 2021.
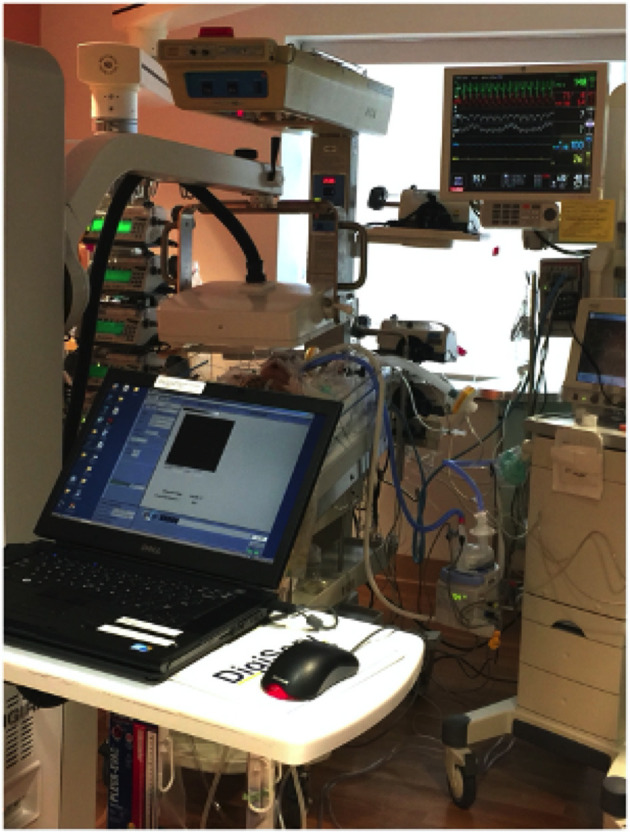
Infants undergoing congenital cardiac surgery with cardiopulmonary bypass are at high risk for respiratory complications. As impaired airway mucociliary clearance (MCC) can potentially contribute to pulmonary morbidity, our study objective was to measure airway clearance in infants undergoing congenital cardiac surgery and examine correlation with clinical covariables that may impair airway clearance function. Airway clearance in infants was measured over 30 min using inhaled nebulized Technetium 99m sulfur colloid administered either via a nasal cannula or the endotracheal tube in intubated infants. This was conducted bedside with a portable gamma camera. No difficulty was encountered in positioning the gamma camera over the patient, and neither the camera nor the MCC scan interfered with routine medical care or caused any adverse events. Patient and perioperative variables were examined relative to the MCC measurements. We prospectively enrolled 57 infants undergoing congenital cardiac surgery and conducted a single MCC scan per patient. MCC data from 42 patients were analyzable, including five pre-operative, 15 (40.5%) in the immediate post-operative period (days 1-2), and 22 (59.5%) were later post-operative (≥3 days). Pre-operative MCC was inversely proportional to days requiring post-operative mechanical ventilation ( = 0.006) and non-invasive positive pressure ventilation ( = 0.017). MCC was higher at later post-operative days ( = 0.002) with immediate post-operative MCC being lower (3%; 0-13%) than either pre-operative (21%; 4-25%) ( = 0.091) or later post-operative MCC (18%; 0-29%) ( = 0.054). Among the infants with low post-operative MCC, significantly more were pre-mature [5/19 (26%) vs. 0/18 (0%); = 0.046], were intubated [14/19 (75%) vs. only 7/18 (39%); = 0.033] and were receiving higher FiO (40%, 27-47% vs. 26%, 21-37%; = 0.015). This is the first study to show that infants undergoing congenital cardiac surgery have impaired MCC. MCC appeared lowest in the immediate post-operative period. Worse MCC was associated with pre-maturity, mechanical ventilation, or receiving higher FiO. These findings suggest MCC scans should be further explored for informing clinical decision making to improve post-surgical respiratory outcomes. The possible therapeutic benefit of airway clearance maneuvers for infants with poor MCC function should also be investigated.
接受体外循环先天性心脏手术的婴儿发生呼吸并发症的风险很高。由于气道黏液纤毛清除功能(MCC)受损可能会导致肺部发病,我们的研究目的是测量接受先天性心脏手术的婴儿的气道清除功能,并研究其与可能损害气道清除功能的临床协变量之间的相关性。对于婴儿,使用通过鼻导管或给插管婴儿经气管内导管吸入雾化的锝99m硫胶体,在30分钟内测量气道清除功能。这是在床边使用便携式伽马相机进行的。将伽马相机放置在患者上方没有遇到困难,并且相机和MCC扫描均未干扰常规医疗护理或引起任何不良事件。针对MCC测量结果检查了患者和围手术期变量。我们前瞻性地纳入了57例接受先天性心脏手术的婴儿,每位患者进行一次MCC扫描。42例患者的MCC数据可进行分析,包括5例术前、15例(40.5%)术后即刻(第1 - 2天)以及22例(59.5%)术后较晚时间(≥3天)。术前MCC与术后需要机械通气的天数(r = 0.006)和无创正压通气的天数(r = 0.017)呈负相关。术后较晚时间的MCC较高(r = 0.002),术后即刻的MCC较低(3%;0 - 13%),低于术前(21%;4 - 25%)(r = 0.091)或术后较晚时间(r = 0.054)的MCC(18%;0 - 29%)。在术后MCC较低的婴儿中,早产的婴儿明显更多[5/19(26%)对0/18(0%);p = 0.046],插管的婴儿更多[14/19(75%)对仅7/18(39%);p = 0.033],并且接受的FiO₂更高(40%,27 - 47%对26%,21 - 37%;p = 0.015)。这是第一项表明接受先天性心脏手术的婴儿存在MCC受损的研究。MCC在术后即刻似乎最低。较差的MCC与早产、机械通气或接受更高的FiO₂有关。这些发现表明,应进一步探索MCC扫描以指导临床决策,改善术后呼吸结局。还应研究气道清除操作对MCC功能不佳的婴儿可能的治疗益处。