Bergen Centre for Ethics and Priority Setting, Department of Global Public Health and Primary Care, University of Bergen, Pb. 7804, 5020, Bergen, Norway.
Centre for Cancer Biomarkers, Department of Global Public Health and Primary Care, University of Bergen, 5020, Bergen, Norway.
BMC Med Ethics. 2021 May 10;22(1):55. doi: 10.1186/s12910-021-00625-3.
In precision medicine biomarkers stratify patients into groups that are offered different treatments, but this may conflict with the principle of equal treatment. While some patient characteristics are seen as relevant for unequal treatment and others not, it is known that they all may influence treatment decisions. How biomarkers influence these decisions is not known, nor is their ethical relevance well discussed.
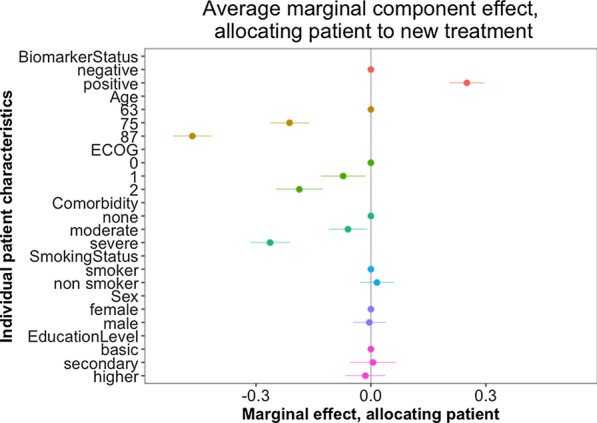
We distributed an email survey designed to elicit treatment preferences from Norwegian doctors working with cancer patients. In a forced-choice conjoint analysis pairs of hypothetical patients were presented, and we calculated the average marginal component effect of seven individual patient characteristics, to estimate how each of them influence doctors' priority-setting decisions.
A positive biomarker status increased the probability of being allocated the new drug, while older age, severe comorbidity and reduced physical function reduced the probability. Importantly, sex, education level and smoking status had no significant influence on the decision.
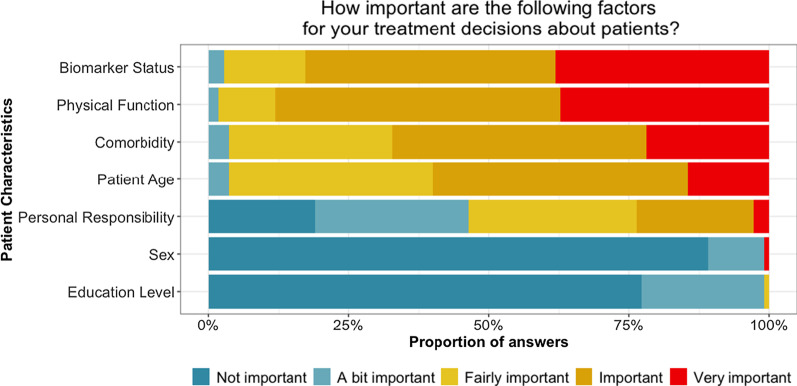
Biomarker status is perceived as relevant for priority setting decisions, alongside more well-known patient characteristics like age, physical function and comorbidity. Based on our results, we discuss a framework that can help clarify whether biomarker status should be seen as an ethically acceptable factor for providing unequal treatment to patients with the same disease.
在精准医学中,生物标志物将患者分为接受不同治疗的群体,但这可能与平等对待的原则相冲突。虽然一些患者特征被认为与不平等对待有关,而另一些则不然,但已知它们都可能影响治疗决策。生物标志物如何影响这些决策尚不清楚,其伦理相关性也未得到充分讨论。
我们分发了一封电子邮件调查,旨在征求挪威癌症患者治疗的医生的治疗偏好。在强制性选择联合分析中,我们呈现了一对假设的患者,并计算了七个个体患者特征的平均边际成分效应,以估计它们中的每一个如何影响医生的优先级设置决策。
阳性生物标志物状态增加了分配新药的概率,而年龄较大、严重合并症和身体功能降低则降低了概率。重要的是,性别、教育水平和吸烟状况对决策没有显著影响。
生物标志物状态被认为与优先级设置决策相关,与年龄、身体功能和合并症等更知名的患者特征并列。基于我们的结果,我们讨论了一个框架,可以帮助澄清生物标志物状态是否应被视为为患有相同疾病的患者提供不平等对待的一个可接受的因素。