Duke University School of Medicine, Durham, North Carolina.
University of North Carolina, Chapel Hill.
Arthritis Care Res (Hoboken). 2022 Oct;74(10):1659-1666. doi: 10.1002/acr.24643. Epub 2022 Jun 28.
To determine the incidence and worsening of lumbar spine structure and low back pain (LBP) and whether they are predicted by demographic characteristics or clinical characteristics or appendicular joint osteoarthritis (OA).
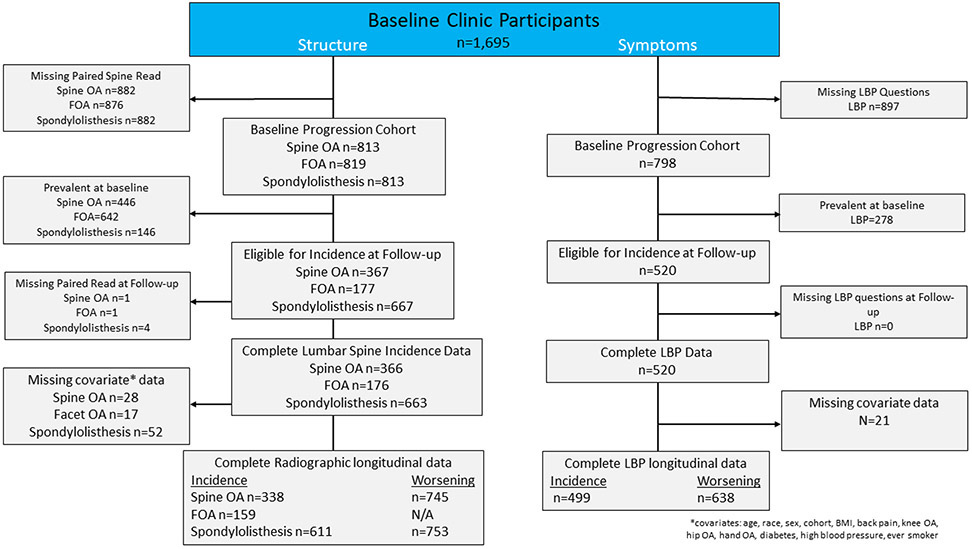
Paired baseline (2003-2004) and follow-up (2006-2010) lumbar spine radiographs from the Johnston County Osteoarthritis Project were graded for osteophytes (OST), disc space narrowing (DSN), spondylolisthesis, and presence of facet joint OA (FOA). Spine OA was defined as at least mild OST and mild DSN at the same level for any level of the lumbar spine. LBP, comorbidities, and back injury were self-reported. Weibull models were used to estimate hazard ratios (HRs) and 95% confidence intervals (95% CIs) of spine phenotypes accounting for potential predictors including demographic characteristics, clinical characteristics, comorbidities, obesity, and appendicular OA.
Obesity was a consistent and strong predictor of incidence of DSN (HR 1.80 [95% CI 1.09-2.98]), spine OA (HR 1.56 [95% CI 1.01-2.41]), FOA (HR 4.99 [95% CI 1.46-17.10]), spondylolisthesis (HR 1.87 [95% CI 1.02-3.43]), and LBP (HR 1.75 [95% CI 1.19-2.56]), and worsening of DSN (HR 1.51 [95% CI 1.09-2.09]) and LBP (HR 1.51 [95% CI 1.12-2.06]). Knee OA was a predictor of incident FOA (HR 4.18 [95% CI 1.44-12.2]). Spine OA (HR 1.80 [95% CI 1.24-2.63]) and OST (HR 1.85 [95% CI 1.02-3.36]) were predictors of incidence of LBP. Hip OA (HR 1.39 [95% CI 1.04-1.85]) and OST (HR 1.58 [95% CI 1.00-2.49]) were predictors of LBP worsening.
Among the multiple predictors of spine phenotypes, obesity was a common predictor for both incidence and worsening of lumbar spine degeneration and LBP.
确定腰椎结构和腰痛(LBP)的发生率和恶化情况,以及它们是否由人口统计学特征或临床特征或附肢关节骨关节炎(OA)预测。
对约翰斯顿县骨关节炎项目的基线(2003-2004 年)和随访(2006-2010 年)腰椎 X 线片进行配对,分级为骨赘(OST)、椎间盘狭窄(DSN)、脊椎滑脱和存在小面关节 OA(FOA)。腰椎 OA 定义为至少有轻度 OST 和同一水平的轻度 DSN,且腰椎任何水平均有轻度 DSN。腰痛、合并症和背部损伤为自我报告。使用威布尔模型估计考虑到潜在预测因素(包括人口统计学特征、临床特征、合并症、肥胖和附肢 OA)的脊柱表型的风险比(HR)和 95%置信区间(95%CI)。
肥胖是 DSN 发生率(HR 1.80[95%CI 1.09-2.98])、脊柱 OA(HR 1.56[95%CI 1.01-2.41])、FOA(HR 4.99[95%CI 1.46-17.10])、脊椎滑脱(HR 1.87[95%CI 1.02-3.43])和 LBP(HR 1.75[95%CI 1.19-2.56])以及 DSN 恶化(HR 1.51[95%CI 1.09-2.09])和 LBP 恶化(HR 1.51[95%CI 1.12-2.06])的一致且强有力的预测因素。膝关节 OA 是 FOA 新发病例的预测因素(HR 4.18[95%CI 1.44-12.2])。脊柱 OA(HR 1.80[95%CI 1.24-2.63])和 OST(HR 1.85[95%CI 1.02-3.36])是 LBP 新发病例的预测因素。髋关节 OA(HR 1.39[95%CI 1.04-1.85])和 OST(HR 1.58[95%CI 1.00-2.49])是 LBP 恶化的预测因素。
在多种脊柱表型预测因素中,肥胖是腰椎退变和 LBP 发生率和恶化的共同预测因素。