Department of Microbiology, Immunology & Molecular Genetics, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA.
Office of the Clinical Director, National Human Genome Research Institute, National Institutes of Health, Bethesda, MD.
Blood. 2021 Oct 14;138(15):1304-1316. doi: 10.1182/blood.2020010260.
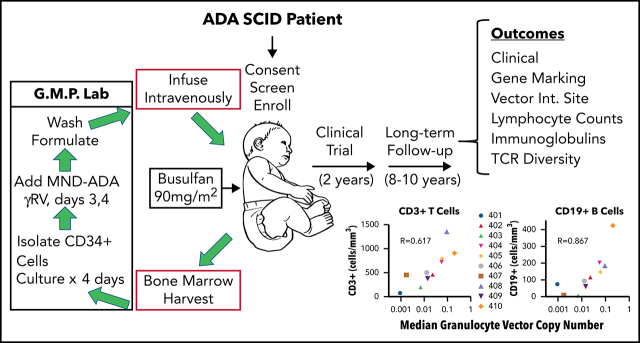
Patients lacking functional adenosine deaminase activity have severe combined immunodeficiency (ADA SCID), which can be treated with ADA enzyme replacement therapy (ERT), allogeneic hematopoietic stem cell transplantation (HSCT), or autologous HSCT with gene-corrected cells (gene therapy [GT]). A cohort of 10 ADA SCID patients, aged 3 months to 15 years, underwent GT in a phase 2 clinical trial between 2009 and 2012. Autologous bone marrow CD34+ cells were transduced ex vivo with the MND (myeloproliferative sarcoma virus, negative control region deleted, dl587rev primer binding site)-ADA gammaretroviral vector (gRV) and infused following busulfan reduced-intensity conditioning. These patients were monitored in a long-term follow-up protocol over 8 to 11 years. Nine of 10 patients have sufficient immune reconstitution to protect against serious infections and have not needed to resume ERT or proceed to secondary allogeneic HSCT. ERT was restarted 6 months after GT in the oldest patient who had no evidence of benefit from GT. Four of 9 evaluable patients with the highest gene marking and B-cell numbers remain off immunoglobulin replacement therapy and responded to vaccines. There were broad ranges of responses in normalization of ADA enzyme activity and adenine metabolites in blood cells and levels of cellular and humoral immune reconstitution. Outcomes were generally better in younger patients and those receiving higher doses of gene-marked CD34+ cells. No patient experienced a leukoproliferative event after GT, despite persisting prominent clones with vector integrations adjacent to proto-oncogenes. These long-term findings demonstrate enduring efficacy of GT for ADA SCID but also highlight risks of genotoxicity with gRVs. This trial was registered at www.clinicaltrials.gov as #NCT00794508.
10 名腺苷脱氨酶(ADA)缺乏功能活性的严重联合免疫缺陷(ADA-SCID)患者参与了 2009 年至 2012 年期间进行的 2 期临床试验,接受了基因治疗(GT)。这些患者的年龄在 3 个月至 15 岁之间,自体骨髓 CD34+细胞在体外经 MND(髓性肉瘤病毒,缺失负调控区,dl587rev 引物结合位点)-ADA γ逆转录病毒载体(gRV)转导,并在白消安降低强度预处理后输注。这些患者在长达 8 至 11 年的长期随访方案中进行监测。在 10 名患者中,有 9 名患者的免疫重建足够,可以预防严重感染,并且无需重新开始 ERT 或进行二次异基因造血干细胞移植。在 GT 后 6 个月,最年长的患者因 GT 无获益而重新开始 ERT。在 9 名可评估的患者中,有 4 名患者的基因标记和 B 细胞数量最高,他们无需免疫球蛋白替代治疗,并且对疫苗有反应。ADA 酶活性和血液细胞中腺嘌呤代谢物以及细胞和体液免疫重建水平的正常化程度存在广泛的差异。在年轻患者和接受更高剂量基因标记 CD34+细胞的患者中,结果通常更好。尽管存在邻近原癌基因的载体整合的明显克隆,但 GT 后没有患者发生白细胞增生性事件。这些长期发现表明 GT 对 ADA-SCID 具有持久疗效,但也强调了 gRV 的遗传毒性风险。该试验在 www.clinicaltrials.gov 上注册,编号为 #NCT00794508。