Yang Xiangwei, Jiang Donggen, Li Yamei, Zhang Tianzhi, Xu Duanya, Chen Xianju, Pang Jun
Department of Urology, Kidney and Urology Center, Pelvic Floor Disorders Center, The Seventh Affiliated Hospital, Sun Yat-Sen University, Shenzhen, China.
Department of Pathology, The Seventh Affiliated Hospital, Sun Yat-Sen University, Shenzhen, China.
Front Oncol. 2021 Apr 26;11:659442. doi: 10.3389/fonc.2021.659442. eCollection 2021.
Prostate cancer (PCa) is the second most common cancer among males in the world and the majority of patients will eventually progress to the metastatic phase. How to choose an effective way for the treatment of metastatic PCa, especially in the later stage of the disease is still confusing. Herein we reported the case of a patient diagnosed with metastatic PCa and conducted a literature review on this issue.
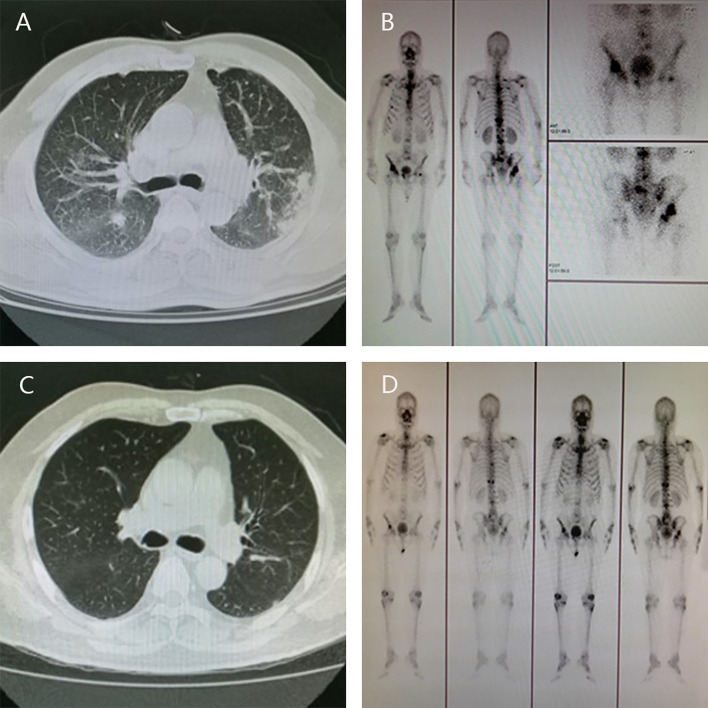
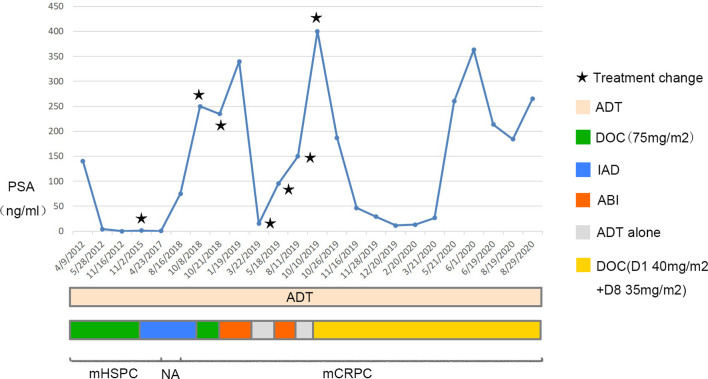
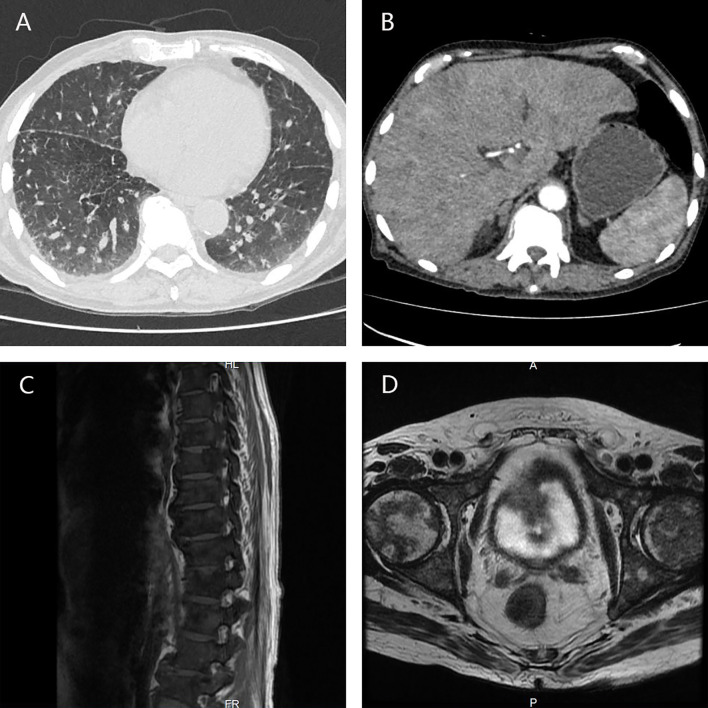
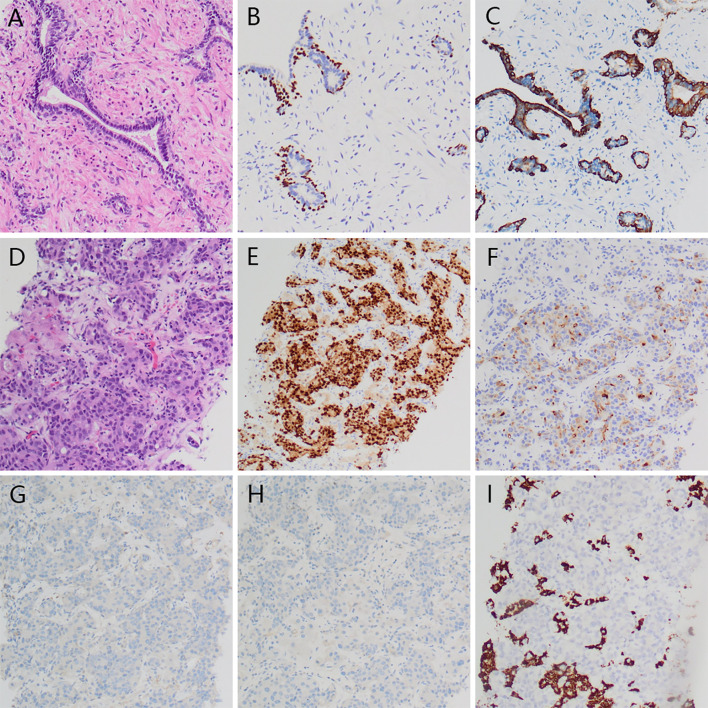
A 57-year-old man with metastatic PCa had been managed by Dr. J.P. since April 2012 when the patient was admitted to the Third Affiliated Hospital of Sun Yat-sen University by aggravating frequent urination and dysuria. The prostate-specific antigen (PSA) concentration was 140 ng/ml, and the diagnosis of PCa was confirmed by prostate biopsy, with Gleason score 4 + 5 = 9. Chest CT and bone scan indicated multiple metastases in the lungs and bones. Triptorelin, bicalutamide, zoledronic acid, and docetaxel were then administered, six cycles later, the metastatic tumors in the lungs disappeared and those in the bones lessened significantly, along with a remarkable reduction in PSA level (< 2 ng/ml). Intermittent androgen deprivation was subsequently conducted until August 2018, when the serum PSA level was found to be 250 ng/ml, again docetaxel 75 mg/m was administered immediately but the patient was intolerant this time. Instead, abiraterone was administered until March 2019 because of intolerable gastrointestinal side-effects and increasing PSA level. In October 2019, the patient came to our center, a modified approach of docetaxel (day 1 40 mg/m + day 8 35 mg/m) was administered. Luckily, the PSA level decreased rapidly, the bone pain was greatly relieved, and no obvious side effects occurred. However, four cycles later, docetaxel failed to work anymore, the metastatic tumor in the liver progressed. We proposed several regimens as alternatives, but they were soon denied due to the high prices or unavailability or uncertain effect of the drugs. In addition, the patient's condition deteriorated speedily and can no longer bear any aggressive treatment. Finally, the patient died of multiple organ failure in August 2020.
The experiences of this case provide valuable evidence and reference for the treatment choices of metastatic PCa, in some circumstances modified and advanced regimens may produce unexpected effects.
前列腺癌(PCa)是全球男性中第二常见的癌症,大多数患者最终会进展到转移阶段。如何选择有效的转移性PCa治疗方法,尤其是在疾病后期,仍然令人困惑。在此,我们报告了一例被诊断为转移性PCa的患者,并对该问题进行了文献综述。
一名患有转移性PCa的57岁男性自2012年4月起由J.P.医生负责治疗,当时患者因尿频和排尿困难加重而入住中山大学附属第三医院。前列腺特异性抗原(PSA)浓度为140 ng/ml,经前列腺活检确诊为PCa,Gleason评分为4 + 5 = 9。胸部CT和骨扫描显示肺部和骨骼有多处转移。随后给予曲普瑞林、比卡鲁胺、唑来膦酸和多西他赛,六个周期后,肺部的转移瘤消失,骨骼中的转移瘤明显缩小,PSA水平显著降低(< 2 ng/ml)。随后进行间歇性雄激素剥夺治疗,直到2018年8月,发现血清PSA水平为250 ng/ml,再次立即给予75 mg/m的多西他赛,但患者这次不耐受。相反,由于无法耐受的胃肠道副作用和PSA水平升高,给予阿比特龙治疗直至2019年3月。2019年10月,患者来到我们中心,给予改良的多西他赛方案(第1天40 mg/m + 第8天35 mg/m)。幸运的是,PSA水平迅速下降,骨痛大大缓解,且未出现明显副作用。然而,四个周期后,多西他赛不再起作用,肝脏中的转移瘤进展。我们提出了几种替代方案,但由于药物价格高、无法获得或效果不确定而很快被否定。此外,患者的病情迅速恶化,无法再承受任何积极的治疗。最后,患者于2020年8月死于多器官功能衰竭。
该病例的经验为转移性PCa的治疗选择提供了有价值的证据和参考,在某些情况下,改良和先进的方案可能会产生意想不到的效果。