Centre for Clinical Epidemiology (Moriello, Reynier, Aibibula, Filion), Lady Davis Institute, Jewish General Hospital, McGill University, Montréal, Que; ICES (Paterson); Institute of Health Policy, Management and Evaluation (Paterson), University of Toronto, Toronto, Ont.; Manitoba Centre for Health Policy, Department of Community Health Sciences (Dahl, Kuo), Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, Man.; Department of Anesthesiology, Pharmacology and Therapeutics (Fisher), University of British Columbia, Vancouver BC; School of Pharmacy (Gamble), University of Waterloo, Kitchener, Ont.; Department of Community Health Sciences (Ronksley), Cumming School of Medicine, University of Calgary, Calgary, Alta.; Saskatchewan Health Quality Council (Winquist); Department of Community Health and Epidemiology (Winquist), College of Medicine, University of Saskatchewan, Saskatoon Sask.; Departments of Medicine and of Epidemiology, Biostatistics, and Occupational Health (Filion), McGill University, Montréal, Que.
CMAJ Open. 2021 May 14;9(2):E500-E509. doi: 10.9778/cmajo.20200084. Print 2021 Apr-Jun.
Trends in off-label postpartum use of domperidone and the impact of safety advisories on its use remain unknown. Our objectives were to describe postpartum use of domperidone in Canada, to evaluate the impact of Health Canada advisories on prescribing patterns, and to describe the association between domperidone use and a composite end point of sudden cardiac death or ventricular tachycardia (VT) among postpartum patients.
We conducted a multidatabase cohort study involving pregnant patients with live births between 2004 and 2017 using administrative health databases from 5 Canadian provinces (British Columbia, Alberta, Saskatchewan, Manitoba and Ontario). We excluded patients with less than 1 year of prepregnancy database history and with approved indications for domperidone. We assessed domperidone use in the 6 months postpartum and the impact of the 2012 and 2015 Health Canada advisories on prescribing via interrupted time series analysis. We estimated crude rates of VT and sudden cardiac death.
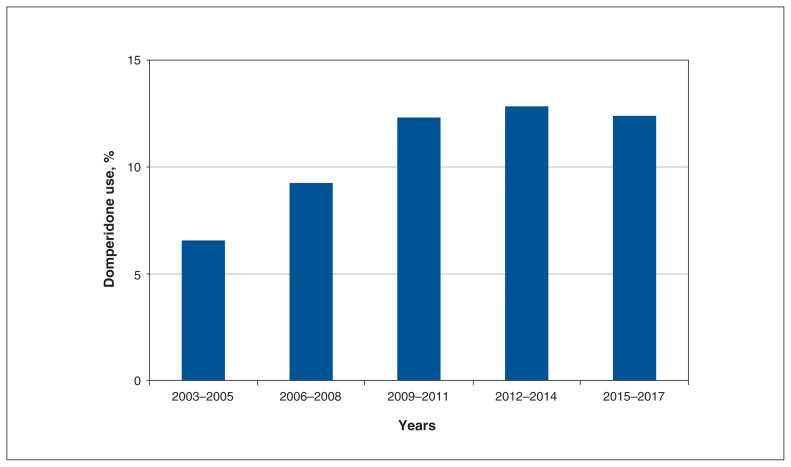
We included 1 190 987 live births. Mean maternal age was 28.6 (standard error 0.6) years. Domperidone use increased over time, from 7% in 2003-2005 to 12% in 2009-2011, when it plateaued. The 2012 advisory was followed by a drop in use and a reduction in slope, and the 2015 advisory had a more modest impact. Crude analysis suggests that domperidone may be associated with increased VT or sudden cardiac death (0.74 v. 0.37 per 10 000 person-years; difference per 10 000 person-years: 0.37, 95% confidence interval -0.67 to 1.41).
Postpartum domperidone use increased between 2004 and 2017, with prescribing attenuated after Health Canada advisories and a very low absolute rate of VT or sudden cardiac death. These findings suggest that Health Canada advisories affected prescribing; any potential increase in VT or sudden cardiac death with use of domperidone is small and could not be confirmed in this large study STUDY REGISTRATION: ClinicalTrials.gov, no. NCT04024865.
多培酮在产后的非适应证使用趋势以及安全性建议对其使用的影响尚不清楚。我们的目标是描述加拿大产后多培酮的使用情况,评估加拿大卫生部建议对处方模式的影响,并描述多培酮使用与产后患者心脏性猝死或室性心动过速(VT)复合终点之间的关系。
我们使用来自加拿大 5 个省(不列颠哥伦比亚省、艾伯塔省、萨斯喀彻温省、马尼托巴省和安大略省)的行政健康数据库,对 2004 年至 2017 年间活产孕妇进行了多数据库队列研究。我们排除了数据库中妊娠前病史少于 1 年和多培酮有适应证的患者。我们通过中断时间序列分析评估了产后 6 个月的多培酮使用情况以及 2012 年和 2015 年加拿大卫生部建议对处方的影响。我们估计了 VT 和心脏性猝死的粗发生率。
我们纳入了 1 190 987 例活产。产妇平均年龄为 28.6(标准误差 0.6)岁。多培酮的使用随着时间的推移而增加,从 2003-2005 年的 7%增加到 2009-2011 年的 12%,之后趋于平稳。2012 年的建议发布后,使用量下降,斜率降低,而 2015 年的建议则产生了更温和的影响。粗略分析表明,多培酮可能与 VT 或心脏性猝死的发生率增加有关(每 10000 人年 0.74 比 0.37;每 10000 人年差异:0.37,95%置信区间 -0.67 至 1.41)。
2004 年至 2017 年间,产后多培酮的使用增加,在加拿大卫生部建议发布后,处方减少,但 VT 或心脏性猝死的绝对发生率非常低。这些发现表明,加拿大卫生部的建议影响了处方;多培酮的使用与 VT 或心脏性猝死的任何潜在增加都很小,在这项大型研究中无法得到证实。
ClinicalTrials.gov,编号 NCT04024865。