Granell Gil M, Sanchís López N, Aldecoa Álvarez de Santulano C, de Andrés Ibáñez J A, Monedero Rodríguez P, Álvarez Escudero J, Rubini Puig R, Romero García C S
Servicio de Anestesiología, Reanimación y T. Dolor, Consorcio General Universitario de Valencia, España.
Facultad de Medicina y Odontología, Universitat de Valencia, Valencia, España.
Rev Esp Anestesiol Reanim. 2022 Jan;69(1):12-24. doi: 10.1016/j.redar.2021.01.005. Epub 2021 Mar 24.
We explored the experience of clinicians from the Spanish Society of Anesthesiology in airway management of COVID-19 patients.
An software-based survey including a 32-item questionnaire was conducted from April 18 to May 17, 2020. Participants who have been involved in tracheal intubations in patients with suspected or confirmed COVID-19 infection were included anonymously after obtaining their informed consent. The primary outcome was the preferred airway device for tracheal intubation. Secondary outcomes included the variations in clinical practice including the preferred video laryngoscope, plans for difficult airway management, and personal protective equipment.
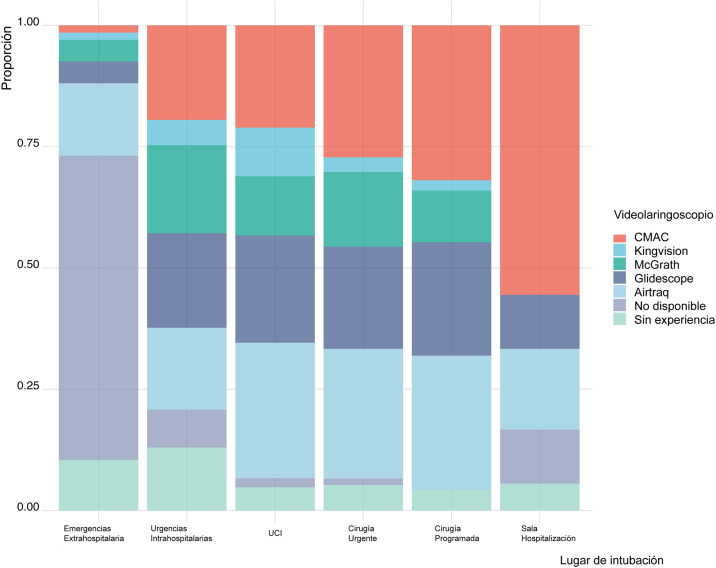
1125 physicians completed the questionnaire with a response rate of 40,9%. Most participants worked in public hospitals and were anesthesiologists.The preferred device for intubation was the video laryngoscope (5.1/6), with the type of device in decreasing order as follows: Glidescope, C-MAC, Airtraq, McGrath and King Vision. The most frequently used device for intubation was the video laryngoscope (70,5%), using them in descending order as follow: the Airtraq, C-MAC, Glidescope, McGrath and King Vision.Discomfort of intubating wearing personal protective equipment and the frequency of breaching a security step was statistically significant, increasing the risk of cross infection between patients and physicians. The opinion of senior doctors differed from younger physicians in the type of video-laryngoscope used, the number of experts involved in tracheal intubation and the reason that caused more stress during the airway management.
Most physicians preferred using a video-laryngoscope with remote monitor and disposable Macintosh blade, using the Frova guide.
我们探讨了西班牙麻醉学会临床医生在新冠病毒疾病(COVID - 19)患者气道管理方面的经验。
于2020年4月18日至5月17日进行了一项基于软件的调查,其中包括一份32项问题的问卷。在获得疑似或确诊COVID - 19感染患者气管插管经验的参与者在获得知情同意后匿名纳入。主要结果是气管插管首选的气道装置。次要结果包括临床实践中的差异,包括首选的视频喉镜、困难气道管理计划以及个人防护装备。
1125名医生完成了问卷,回复率为40.9%。大多数参与者在公立医院工作且为麻醉医生。插管的首选装置是视频喉镜(5.1/6),装置类型按使用频率从高到低依次为:Glidescope、C - MAC、Airtraq、McGrath和King Vision。最常使用的插管装置是视频喉镜(70.5%),使用频率从高到低依次为:Airtraq、C - MAC、Glidescope、McGrath和King Vision。穿着个人防护装备进行插管时的不适感以及违反安全步骤的频率具有统计学意义,增加了患者与医生之间交叉感染的风险。在使用的视频喉镜类型、参与气管插管的专家数量以及气道管理过程中造成更多压力的原因方面,资深医生与年轻医生的意见存在差异。
大多数医生更喜欢使用带有远程监视器和一次性麦氏叶片的视频喉镜,并使用弗罗瓦导丝。