Javed Saad, Koniari Ioanna, Fox David, Skene Chris, Lip Gregory Yh, Gupta Dhiraj
Liverpool Centre for Cardiovascular Science, University of Liverpool, Liverpool Heart and Chest Hospital, Liverpool, UK.
Division of Cardiovascular Sciences, University of Manchester, Manchester, UK.
J Geriatr Cardiol. 2021 Apr 28;18(4):297-306. doi: 10.11909/j.issn.1671-5411.2021.04.002.
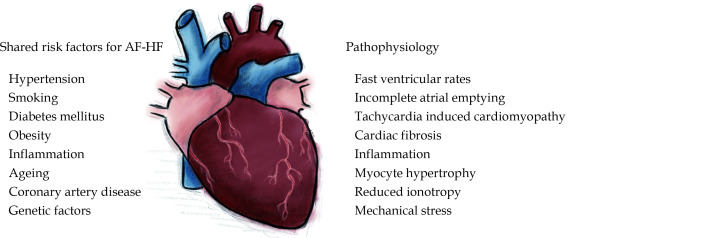
Atrial fibrillation (AF) and heart failure (HF) are complex clinical entities that occur concomitantly in a significant population of patients, and their prevalence is rising in epidemic proportions. Traditionally, both rate and rhythm control strategies have been regarded as equivalent in the management of dysrhythmia in this AF-HF cohort with escalation of treatment largely guided by symptoms. Both disorders are involved in an elaborate pathophysiological interplay with shared cardiovascular risk factors that contribute to the development and sustenance of both AF and HF. Recent studies and continued development of evidence to support catheter ablation for AF has brought into question the traditional belief in equivalence between rate and rhythm control. Indeed, recent trials, in particular the CASTLE-AF (Catheter Ablation versus Standard Conventional Therapy in Patients with Left Ventricular Dysfunction and Atrial Fibrillation) study, suggest that catheter ablation for AF improves survival and rates of hospitalisation in patients with concomitant HF and AF, threatening a paradigm shift in the management of this patient cohort. The evident mortality benefit from clinical trials suggests that catheter ablation for AF should be considered as a therapeutic intervention in all suitable patients with the AF-HF syndrome as these patients may derive the greatest benefit from restoration of sinus rhythm. Further research is needed to refine the evidence base, especially to determine which subgroup of HF patients benefit most from catheter ablation and what is the optimal timing.
心房颤动(AF)和心力衰竭(HF)是复杂的临床病症,在相当一部分患者中同时出现,且其患病率正呈流行趋势上升。传统上,在这一AF-HF队列中,心率控制和节律控制策略在心律失常管理方面被视为等效,治疗升级主要由症状引导。这两种病症都参与了与共同心血管危险因素的复杂病理生理相互作用,这些因素促成了AF和HF的发生与维持。最近的研究以及支持AF导管消融的证据不断发展,使人们对心率控制和节律控制等效的传统观念产生了质疑。事实上,最近的试验,特别是CASTLE-AF(左心室功能障碍合并心房颤动患者的导管消融与标准传统治疗)研究表明,AF导管消融可提高合并HF和AF患者的生存率及住院率,这可能会改变这一患者队列的管理模式。临床试验中明显的死亡率获益表明,对于所有合适的AF-HF综合征患者,AF导管消融应被视为一种治疗干预措施,因为这些患者可能从恢复窦性心律中获得最大益处。需要进一步研究以完善证据基础,特别是确定哪些HF患者亚组从导管消融中获益最大以及最佳时机是什么。