Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Bandung 45363, Indonesia.
Center of Excellence in Higher Education for Pharmaceutical Care Innovation, Universitas Padjadjaran, Bandung 45363, Indonesia.
J Environ Public Health. 2021 Apr 27;2021:7494965. doi: 10.1155/2021/7494965. eCollection 2021.
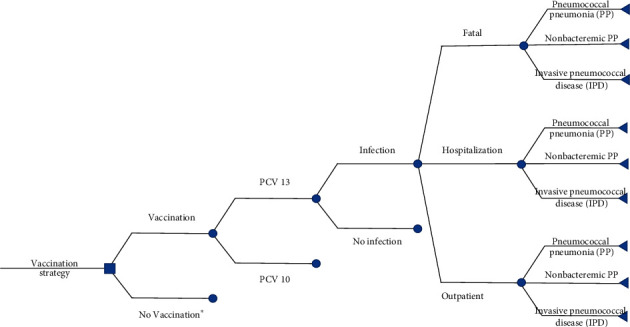
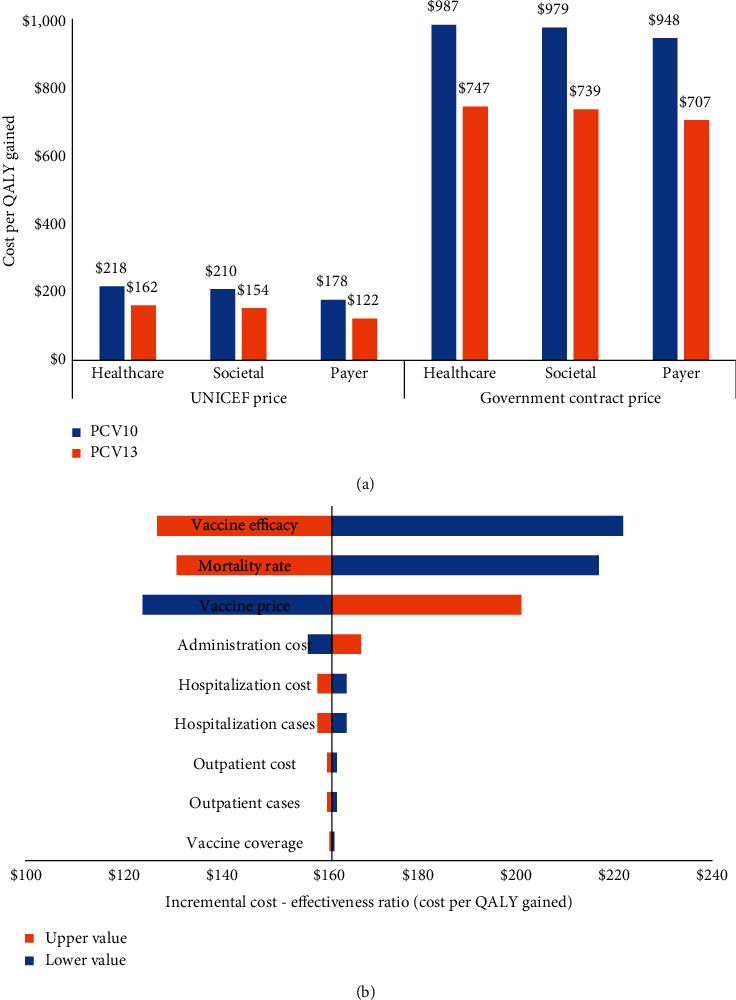
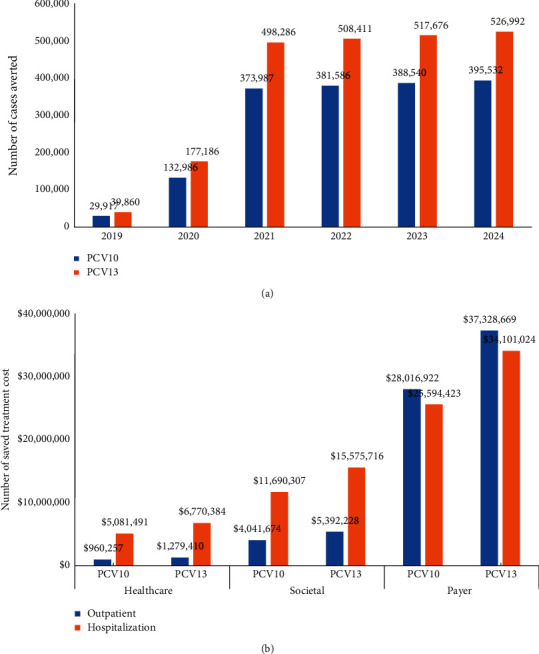
As a country with the high number of deaths due to pneumococcal disease, Indonesia has not yet included pneumococcal vaccination into the routine program. This study aimed to analyse the cost-effectiveness and the budget impact of pneumococcal vaccination in Indonesia by developing an age-structured cohort model. In a comparison with no vaccination, the use of two vaccines (PCV10 and PCV13) within two pricing scenarios (UNICEF and government contract price) was taken into account. To estimate the cost-effectiveness value, a 5-year time horizon was applied by extrapolating the outcome of the individual in the modelled cohort until 5 years of age with a 1-month analytical cycle. To estimate the affordability value, a 6-year period (2019-2024) was applied by considering the government's strategic plan on pneumococcal vaccination. In a comparison with no vaccination, the results showed that vaccination would reduce pneumococcal disease by 1,702,548 and 2,268,411 cases when using PCV10 and PCV13, respectively. Vaccination could potentially reduce the highest treatment cost from the payer perspective at $53.6 million and $71.4 million for PCV10 and PCV13, respectively. Applying the UNICEF price, the incremental cost-effectiveness ratio (ICER) from the healthcare perspective would be $218 and $162 per QALY-gained for PCV10 and PCV13, respectively. Applying the government contract price, the ICER would be $987 and $747 per QALY-gained for PCV10 and PCV13, respectively. The result confirmed that PCV13 was more cost-effective than PCV10 with both prices. In particular, introduction cost per child was estimated to be $0.91 and vaccination cost of PCV13 per child (3 doses) was estimated to be $16.61 and $59.54 with UNICEF and government contract prices, respectively. Implementation of nationwide vaccination would require approximately $73.3-$75.0 million (13-14% of routine immunization budget) and $257.4-$263.5 million (45-50% of routine immunization budget) with UNICEF and government contract prices, respectively. Sensitivity analysis showed that vaccine efficacy, mortality rate, and vaccine price were the most influential parameters affecting the ICER. In conclusion, pneumococcal vaccination would be a highly cost-effective intervention to be implemented in Indonesia. Yet, applying PCV13 with UNICEF price would give the best cost-effectiveness and affordability values on the routine immunization budget.
作为一个因肺炎球菌性疾病导致死亡人数较多的国家,印度尼西亚尚未将肺炎球菌疫苗接种纳入常规计划。本研究旨在通过建立年龄结构队列模型,分析印度尼西亚肺炎球菌疫苗接种的成本效益和预算影响。在与不接种疫苗的比较中,考虑了两种疫苗(PCV10 和 PCV13)在两种定价方案(联合国儿童基金会和政府合同价格)下的使用情况。为了估计成本效益值,通过将模型队列中个体的结果外推到 5 岁以下并采用 1 个月的分析周期,应用了 5 年的时间范围。为了估计可负担性值,考虑到政府关于肺炎球菌疫苗接种的战略计划,应用了 6 年的时间(2019-2024 年)。与不接种疫苗相比,结果表明,使用 PCV10 和 PCV13 分别接种疫苗可使肺炎球菌疾病减少 1702548 例和 2268411 例。从付款人的角度来看,接种疫苗可能会降低最高的治疗费用,PCV10 和 PCV13 分别为 5360 万美元和 7140 万美元。采用联合国儿童基金会价格,从医疗保健角度来看,PCV10 和 PCV13 的增量成本效益比(ICER)将分别为每获得 1 个 QALY 支付 218 美元和 162 美元。采用政府合同价格,PCV10 和 PCV13 的 ICER 将分别为每获得 1 个 QALY 支付 987 美元和 747 美元。结果证实,在两种价格下,PCV13 均比 PCV10 更具成本效益。特别是,估计每个孩子的接种引入成本为 0.91 美元,每个孩子(3 剂)的 PCV13 接种成本估计为 16.61 美元和 59.54 美元,分别采用联合国儿童基金会和政府合同价格。在全国范围内实施疫苗接种,采用联合国儿童基金会和政府合同价格,分别需要约 7330 万至 7500 万美元(常规免疫预算的 13-14%)和 25740 万至 26350 万美元(常规免疫预算的 45-50%)。敏感性分析表明,疫苗效力、死亡率和疫苗价格是影响 ICER 的最具影响力的参数。总之,肺炎球菌疫苗接种将是印度尼西亚一项极具成本效益的干预措施。然而,在常规免疫预算方面,采用联合国儿童基金会价格的 PCV13 将提供最佳的成本效益和可负担性价值。