Nasa Prashant, Chaudhary Sandeep, Shrivastava Pavan Kumar, Singh Aanchal
Department of Critical Care Medicine, NMC Specialty Hospital, Dubai 7832, United Arab Emirates.
Department of Endocrinology, NMC Specialty Hospital, Dubai 7832, United Arab Emirates.
World J Diabetes. 2021 May 15;12(5):514-523. doi: 10.4239/wjd.v12.i5.514.
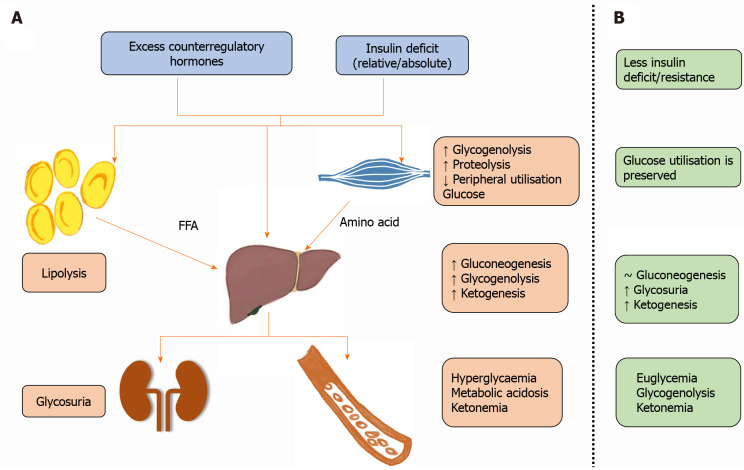
Euglycemic diabetic ketoacidosis (DKA) is an acute life-threatening metabolic emergency characterized by ketoacidosis and relatively lower blood glucose (less than 11 mmol/L). The absence of hyperglycemia is a conundrum for physicians in the emergency department and intensive care units; it may delay diagnosis and treatment causing worse outcomes. Euglycemic DKA is an uncommon diagnosis but can occur in patients with type 1 or type 2 diabetes mellitus. With the addition of sodium/ glucose cotransporter-2 inhibitors in diabetes mellitus management, euglycemic DKA incidence has increased. The other causes of euglycemic DKA include pregnancy, fasting, bariatric surgery, gastroparesis, insulin pump failure, cocaine intoxication, chronic liver disease and glycogen storage disease. The pathophysiology of euglycemic DKA involves a relative or absolute carbohydrate deficit, milder degree of insulin deficiency or resistance and increased glucagon/insulin ratio. Euglycemic DKA is a diagnosis of exclusion and should be considered in the differential diagnosis of a sick patient with a history of diabetes mellitus despite lower blood glucose or absent urine ketones. The diagnostic workup includes arterial blood gas for metabolic acidosis, serum ketones and exclusion of other causes of high anion gap metabolic acidosis. Euglycemic DKA treatment is on the same principles as for DKA with correction of dehydration, electrolytes deficit and insulin replacement. The dextrose-containing fluids should accompany intravenous insulin to correct metabolic acidosis, ketonemia and to avoid hypoglycemia.
正常血糖性糖尿病酮症酸中毒(DKA)是一种急性危及生命的代谢急症,其特征为酮症酸中毒且血糖相对较低(低于11 mmol/L)。无高血糖现象对于急诊科和重症监护病房的医生而言是个难题;这可能会延误诊断和治疗,导致更糟的后果。正常血糖性DKA是一种不常见的诊断,但可发生于1型或2型糖尿病患者。随着糖尿病管理中加入钠/葡萄糖协同转运蛋白-2抑制剂,正常血糖性DKA的发病率有所增加。正常血糖性DKA的其他病因包括妊娠、禁食、减肥手术、胃轻瘫、胰岛素泵故障、可卡因中毒、慢性肝病和糖原贮积病。正常血糖性DKA的病理生理学涉及相对或绝对的碳水化合物缺乏、较轻程度的胰岛素缺乏或抵抗以及胰高血糖素/胰岛素比值增加。正常血糖性DKA是一种排除性诊断,对于有糖尿病病史的患病患者,尽管血糖较低或尿酮阴性,在鉴别诊断时也应考虑。诊断检查包括检测动脉血气以判断是否存在代谢性酸中毒、血清酮,并排除其他导致高阴离子间隙代谢性酸中毒的病因。正常血糖性DKA的治疗原则与DKA相同,即纠正脱水、电解质缺乏并补充胰岛素。含葡萄糖的液体应与静脉胰岛素一同使用,以纠正代谢性酸中毒、酮血症并避免低血糖。