University of Bordeaux, Inserm, French National Research Institute for Sustainable Development (IRD), Bordeaux Population Health Research Center, Team IDLIC, UMR 1219, Bordeaux, France.
The Alliance for International Medical Action (ALIMA), Paris, France.
J Nutr Sci. 2021 Apr 19;10:e27. doi: 10.1017/jns.2021.18. eCollection 2021.
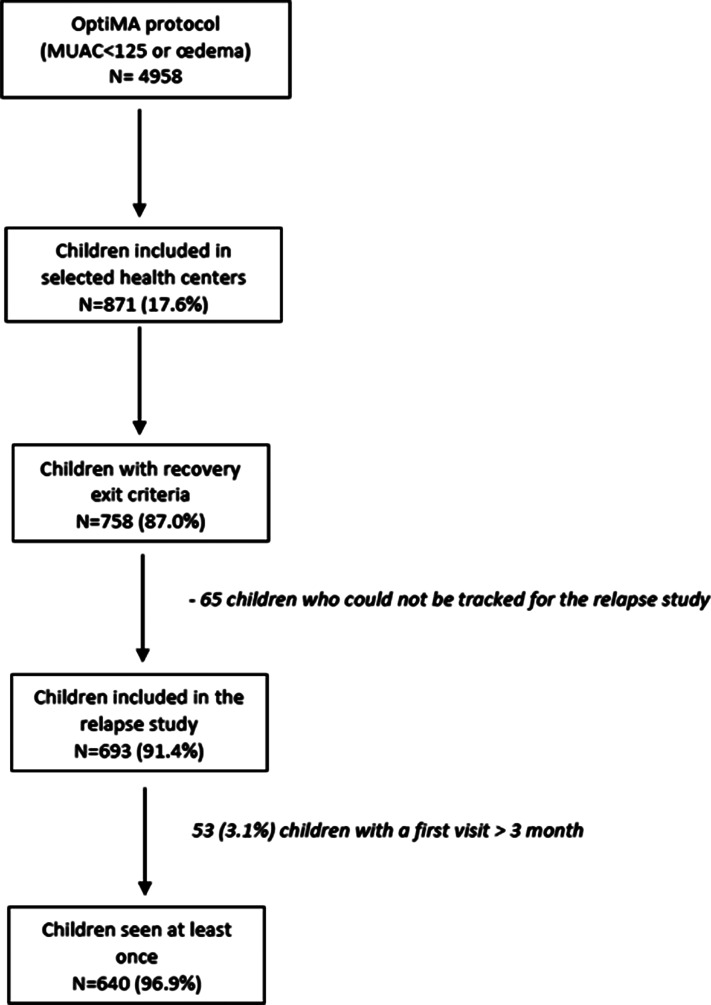
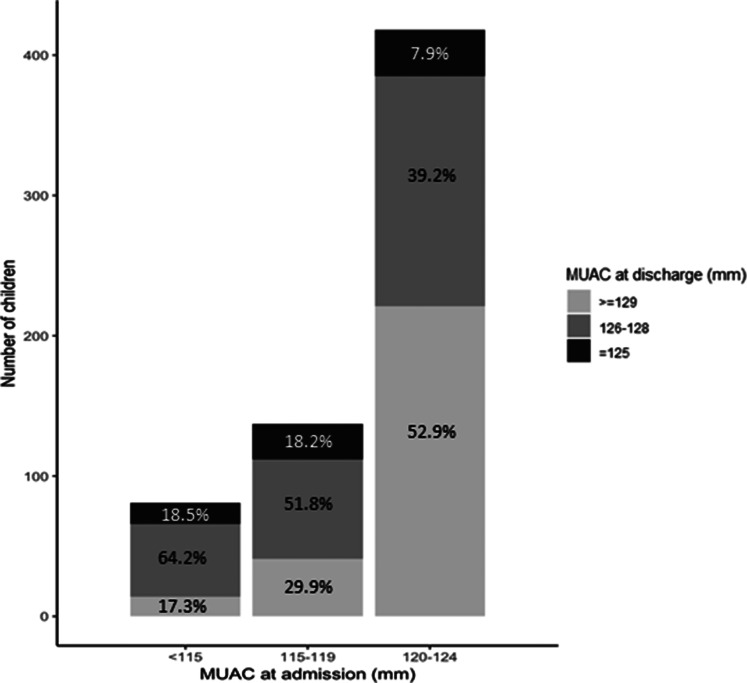
The present study aimed to determine the 3-month incidence of relapse and associated factors among children who recovered under the Optimising treatment for acute MAlnutrition (OptiMA) strategy, a MUAC-based protocol. A prospective cohort of children successfully treated for acute malnutrition was monitored between April 2017 and February 2018. Children were seen at home by community health workers (CHWs) every 2 weeks for 3 months. Relapse was defined as a child who had met OptiMA recovery criteria (MUAC ≥ 125 mm for two consecutive weeks) but subsequently had a MUAC < 125 mm at any home visit. Cumulative incidence and incidence rates per 100 child-months were estimated. Multivariable survival analysis was conducted using a shared frailty model with a random effect on health facilities to identify associated factors. Of the 640 children included, the overall 3-month cumulative incidence of relapse was 6⋅8 % (95 % CI 5⋅2, 8⋅8). Globally, the incidence rate of relapse was 2⋅5 (95 % CI 1⋅9, 3⋅3) per 100 child-months and 3⋅7 (95 % CI 1⋅9, 6⋅8) per 100 child-months among children admitted with a MUAC < 115 mm. Most (88⋅6 %) relapses were detected early when MUAC was between 120 and 124 mm. Relapse was positively associated with hospitalisation, with an adjusted hazard ratio (aHR) of 2⋅06 (95 % CI 1⋅01, 4⋅26) for children who had an inpatient stay at any point during treatment compared with children who did not. The incidence of relapse following recovery under OptiMA was relatively low in this context, but the lack of a standard relapse definition does not allow for comparison across settings Closer follow-up with caretakers whose children are admitted with MUAC < 115 mm or required hospitalisation during treatment should be considered in managing groups at high risk of relapse. Training caretakers to screen their children for relapse at home using MUAC could be more effective at detecting early relapse, and less costly, than home visits by CHWs.
本研究旨在确定在基于 MUAC 的优化急性营养不良治疗(OptiMA)方案下康复的儿童在 3 个月内的复发率及其相关因素。2017 年 4 月至 2018 年 2 月,对成功接受急性营养不良治疗的儿童进行了前瞻性队列研究。由社区卫生工作者(CHW)每两周家访一次,随访 3 个月。复发定义为符合 OptiMA 康复标准(连续两周 MUAC≥125mm)但随后任何家访时 MUAC<125mm 的儿童。估计累计发生率和每 100 儿童-月的发生率。采用具有卫生机构随机效应的共享脆弱性模型进行多变量生存分析,以确定相关因素。在纳入的 640 名儿童中,3 个月的总体累积复发率为 6.8%(95%CI 5.2,8.8)。总体而言,复发率为每 100 儿童-月 2.5(95%CI 1.9,3.3),MUAC<115mm 入院的儿童为每 100 儿童-月 3.7(95%CI 1.9,6.8)。88.6%的复发发生在 MUAC 在 120 至 124mm 之间的早期,大多被早期发现。与未住院的儿童相比,住院治疗的儿童复发的调整后危险比(aHR)为 2.06(95%CI 1.01,4.26)。在这种情况下,OptiMA 治疗后康复的儿童复发率相对较低,但缺乏标准的复发定义,无法在不同环境下进行比较。对于 MUAC<115mm 入院或治疗期间需要住院的儿童,应考虑对其照顾者进行更密切的随访。培训照顾者使用 MUAC 在家中筛查其儿童的复发情况,可能比 CHW 的家访更有效且成本更低。