Action Against Hunger | Action Contre la Faim (ACF) - France, 14-16 Boulevard Douaumont, 75854, Paris, France.
Action Against Hunger | Action Contre la Faim (ACF)- Nepal, Kathmandu, Nepal.
Nutr J. 2021 Apr 5;20(1):32. doi: 10.1186/s12937-021-00684-7.
There is a dearth of evidence on what should be the optimal criteria for discharging children from severe acute malnutrition (SAM) treatment. Programs discharging children while they are still presenting varying levels of weight-for-height (WHZ) or mid-upper-arm circumference (MUAC) deficits, such as those implemented under the current national protocol in Nepal, are opportunities to fill this evidence gap.
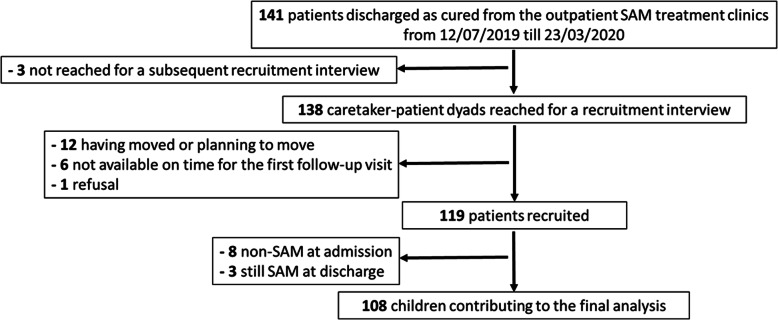
We followed a cohort of children discharged as cured from SAM treatment in Parasi district, Nepal. Relapse as SAM, defined as the occurrence of WHZ<-3 or MUAC < 115 mm or nutritional edema, was investigated through repeated home visits, during six months after discharge. We assessed the contribution of remaining anthropometric deficits at discharge to relapse risk through Cox regressions.
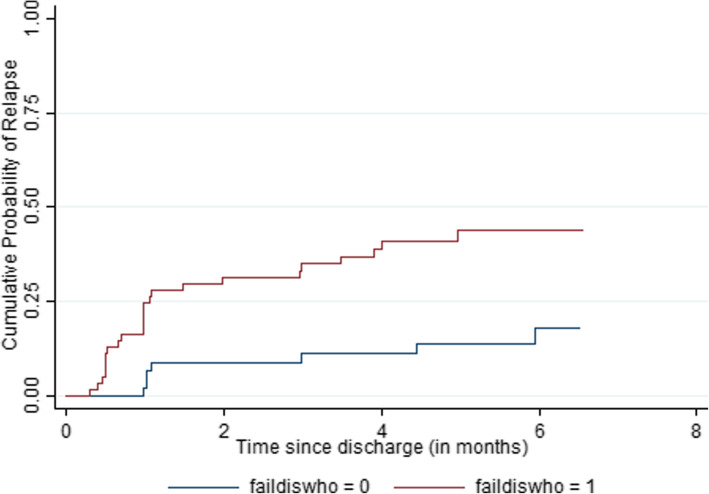
Relapse as SAM during follow-up was observed in 33 % of the cohort (35/108). Being discharged before reaching the internationally recommended criteria was overall associated with a large increase in the risk of relapse (HR = 3.3; p = 0.006). Among all anthropometric indicators at discharge, WHZ<-2 led to a three-fold increase in relapse risk (HR = 3.2; p = 0.003), while MUAC < 125 mm significantly raised it only in the older children. WHZ<-2 at discharge came up as the only significant predictor of relapse in multivariate analysis (HR = 2.8, p = 0.01), even among children with a MUAC ≥ 125 mm. Of note, more than 80 % of the events of relapse as SAM would have been missed if WHZ had not been monitored and used in the definition of relapse.
Our results suggest that the priority for SAM management programs should be to ensure that children reach a high level of WHZ at discharge, at least above or equal to the WHO recommended cut-off. The validity of using a single MUAC cut-off such as 125 mm as a suitable discharge criterion for all age groups is questioned. Further follow-up studies providing a complete assessment of nutritional status at discharge and not based on a restricted MUAC-only definition of relapse as SAM would be urgently needed to set evidence-based discharge criteria. These studies are also required to assess programs currently discounting or omitting WHZ for identification and management of SAM.
目前对于儿童严重急性营养不良(SAM)治疗后应选择哪些最佳标准出院,证据仍十分缺乏。在尼泊尔,现行国家方案下,许多项目都存在出院标准不统一的问题,有些项目在患儿仍存在不同程度的身高体重比(WHZ)或上臂中部周长(MUAC)缺陷时便允许患儿出院,这为填补该证据空白提供了机会。
我们对尼泊尔帕拉西地区从 SAM 治疗中治愈出院的患儿进行了队列研究。通过出院后 6 个月的多次家访,调查了患儿在随访期间因 SAM 复发的情况,定义为 WHZ<-3 或 MUAC<115mm 或出现营养性水肿。我们通过 Cox 回归评估了出院时仍存在的人体测量学缺陷对复发风险的影响。
在随访期间,33%(35/108)的患儿出现了 SAM 复发。与达到国际推荐标准相比,提前出院总体上会大大增加复发风险(HR=3.3,p=0.006)。在所有出院时的人体测量学指标中,WHZ<-2 会使复发风险增加三倍(HR=3.2,p=0.003),而 MUAC<125mm 仅在较大儿童中显著增加了复发风险。WHZ<-2 是多变量分析中唯一显著的复发预测因素(HR=2.8,p=0.01),即使在 MUAC≥125mm 的儿童中也是如此。值得注意的是,如果不监测和使用 WHZ 来定义复发,超过 80%的 SAM 复发事件将被遗漏。
我们的研究结果表明,SAM 管理方案的重点应是确保患儿在出院时达到较高的 WHZ 水平,至少达到或超过世卫组织推荐的截止值。质疑使用单一 MUAC 截止值(如 125mm)作为所有年龄组的合适出院标准的有效性。迫切需要进一步的随访研究,以提供出院时营养状况的全面评估,而不是基于对 SAM 复发的受限 MUAC 定义。这些研究还需要评估目前忽略或省略 WHZ 用于识别和管理 SAM 的方案。