Liu Qin, Li Jie, Xu Lin, Wang Jiasi, Zeng Zhaoping, Fu Jiangping, Huang Xuan, Chu Yanpeng, Wang Jing, Zhang Hong-Yu, Zeng Fanxin
Department of Clinical Research Center, Dazhou Central Hospital, Dazhou, China.
Department of Radiology, Dazhou Central Hospital, Dazhou, China.
Front Oncol. 2021 Apr 28;11:620945. doi: 10.3389/fonc.2021.620945. eCollection 2021.
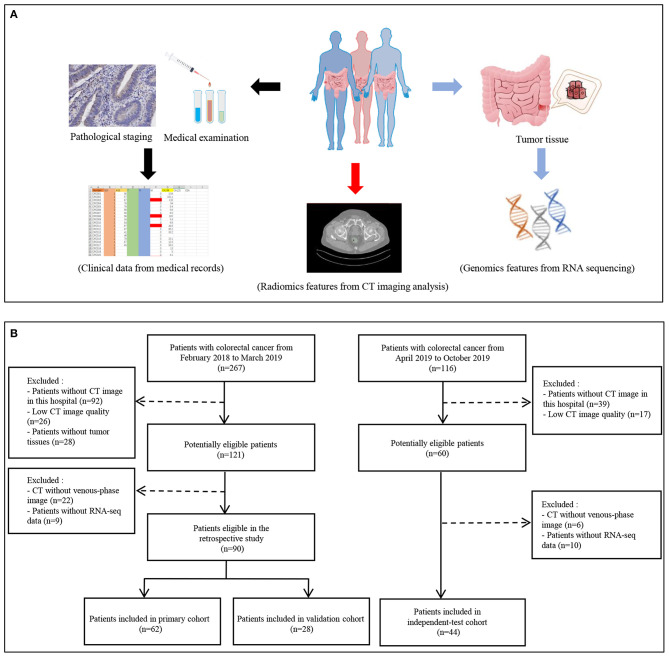
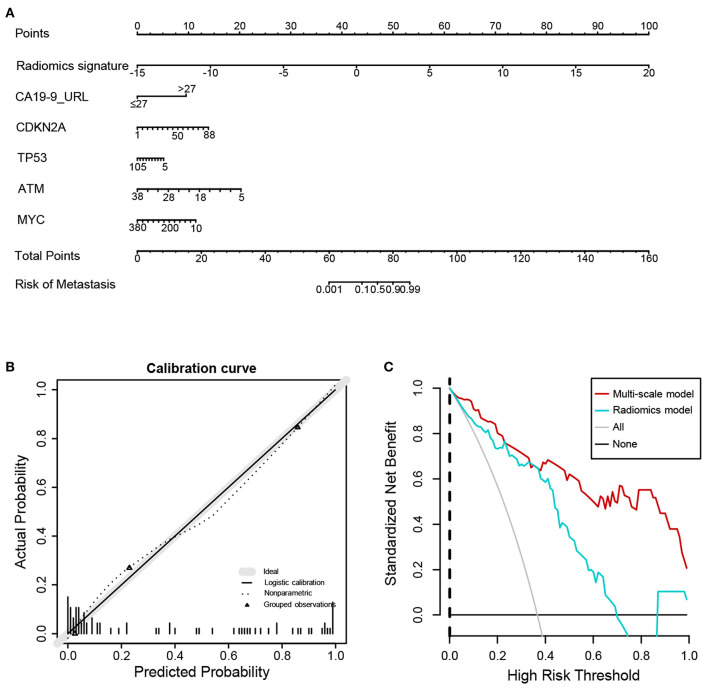
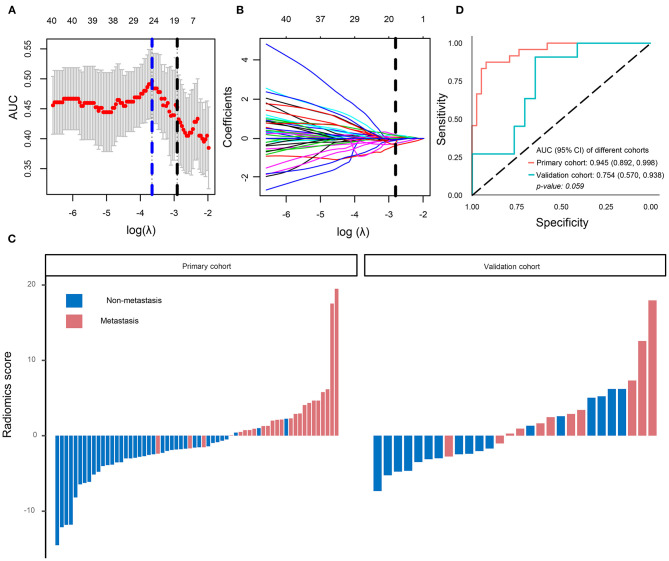
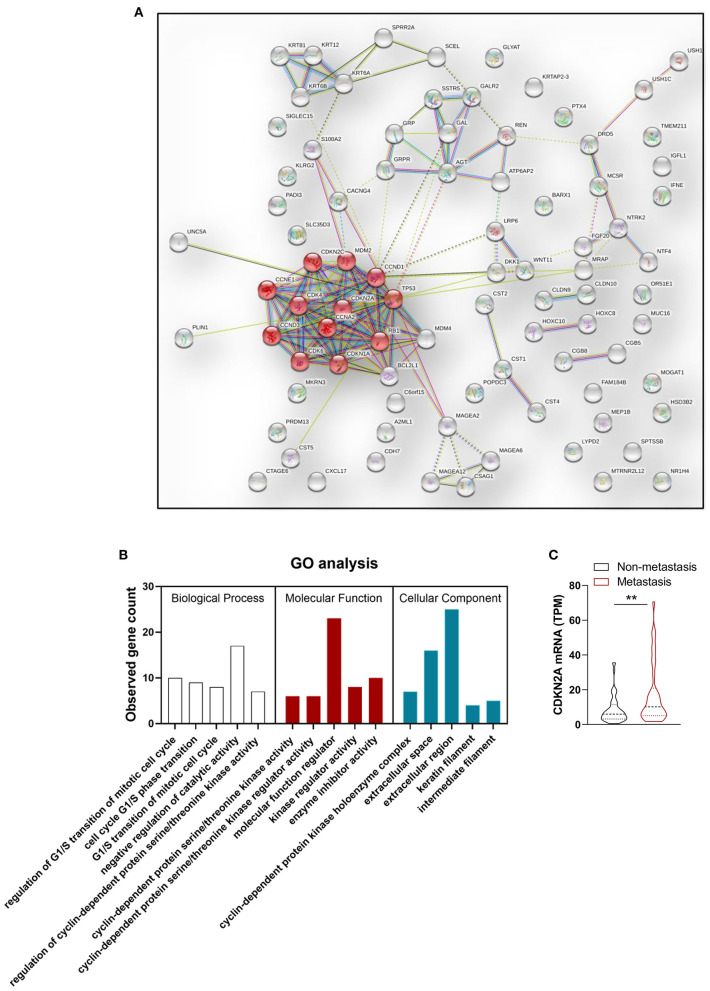
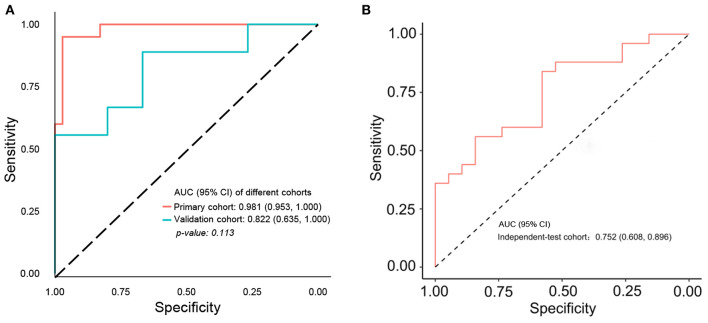
To evaluate whether incorporating the radiomics, genomics, and clinical features allows prediction of metastasis in colorectal cancer (CRC) and to develop a preoperative nomogram for predicting metastasis. We retrospectively analyzed radiomics features of computed tomography (CT) images in 134 patients (62 in the primary cohort, 28 in the validation cohort, and 44 in the independent-test cohort) clinicopathologically diagnosed with CRC at Dazhou Central Hospital from February 2018 to October 2019. Tumor tissues were collected from all patients for RNA sequencing, and clinical data were obtained from medical records. A total of 854 radiomics features were extracted from enhanced venous-phase CT of CRC. Least absolute shrinkage and selection operator regression analysis was utilized for data dimension reduction, feature screen, and radiomics signature development. Multivariable logistic regression analysis was performed to build a multiscale predicting model incorporating the radiomics, genomics, and clinical features. The receiver operating characteristic curve, calibration curve, and decision curve were conducted to evaluate the performance of the nomogram. The radiomics signature based on 16 selected radiomics features showed good performance in metastasis assessment in both primary [area under the curve (AUC) = 0.945, 95% confidence interval (CI) 0.892-0.998] and validation cohorts (AUC = 0.754, 95% CI 0.570-0.938). The multiscale nomogram model contained radiomics features signatures, four-gene expression related to cell cycle pathway, and CA 19-9 level. The multiscale model showed good discrimination performance in the primary cohort (AUC = 0.981, 95% CI 0.953-1.000), the validation cohort (AUC = 0.822, 95% CI 0.635-1.000), and the independent-test cohort (AUC = 0.752, 95% CI 0.608-0.896) and good calibration. Decision curve analysis confirmed the clinical application value of the multiscale model. This study presented a multiscale model that incorporated the radiological eigenvalues, genomics features, and CA 19-9, which could be conveniently utilized to facilitate the individualized preoperatively assessing metastasis in CRC patients.
评估整合放射组学、基因组学和临床特征是否能够预测结直肠癌(CRC)的转移情况,并开发一种用于预测转移的术前列线图。我们回顾性分析了2018年2月至2019年10月在达州中心医院经临床病理诊断为CRC的134例患者(62例在 primary cohort,28例在 validation cohort,44例在 independent - test cohort)的计算机断层扫描(CT)图像的放射组学特征。从所有患者收集肿瘤组织进行RNA测序,并从病历中获取临床数据。从CRC的增强静脉期CT中提取了总共854个放射组学特征。采用最小绝对收缩和选择算子回归分析进行数据降维、特征筛选和放射组学特征开发。进行多变量逻辑回归分析以构建一个整合放射组学、基因组学和临床特征的多尺度预测模型。采用受试者工作特征曲线、校准曲线和决策曲线来评估列线图的性能。基于16个选定放射组学特征的放射组学特征在 primary cohort(曲线下面积[AUC]=0.945,95%置信区间[CI]0.892 - 0.998)和 validation cohort(AUC = 0.754,95% CI 0.570 - 0.938)的转移评估中均表现出良好性能。多尺度列线图模型包含放射组学特征签名、与细胞周期途径相关的四个基因表达以及CA 19 - 9水平。多尺度模型在 primary cohort(AUC = 0.981,95% CI 0.953 - 1.000)、validation cohort(AUC = 0.822,95% CI 0.635 - 1.000)和 independent - test cohort(AUC = 0.752,95% CI 0.608 - 0.896)中表现出良好的区分性能和良好的校准。决策曲线分析证实了多尺度模型的临床应用价值。本研究提出了一种整合放射学特征值、基因组学特征和CA 19 - 9的多尺度模型,可方便地用于促进对CRC患者术前转移情况的个体化评估。