Cai Lianhong, Hu Zhanqi, Liao Jianxiang, Hong Siqi, Kong Lingyu, Chen Li, Luo Yetao, Li Tingsong, Jiang Li
Department of Neurology, Children's Hospital of Chongqing Medical University, Ministry of Education Key Laboratory of Child Development and Disorders, National Clinical Research Center for Child Health and Disorders (Chongqing), International Science and Technology Cooperation Base of Child Development and Critical Disorders, Chongqing Key Laboratory of Pediatrics, Chongqing, China.
Department of Neurology, Shenzhen Children's Hospital, Shenzhen, China.
Front Pediatr. 2021 Apr 29;9:649053. doi: 10.3389/fped.2021.649053. eCollection 2021.
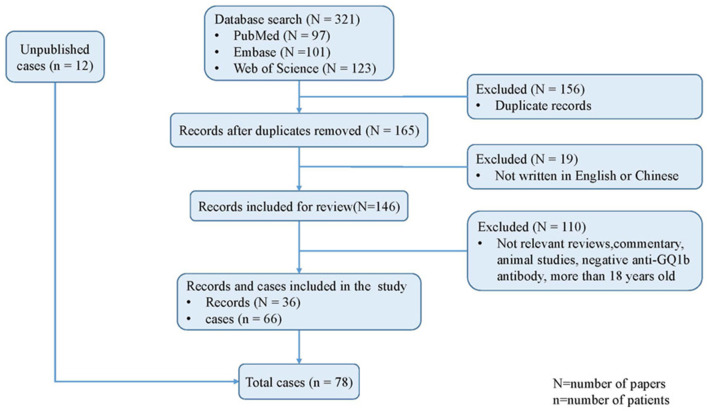
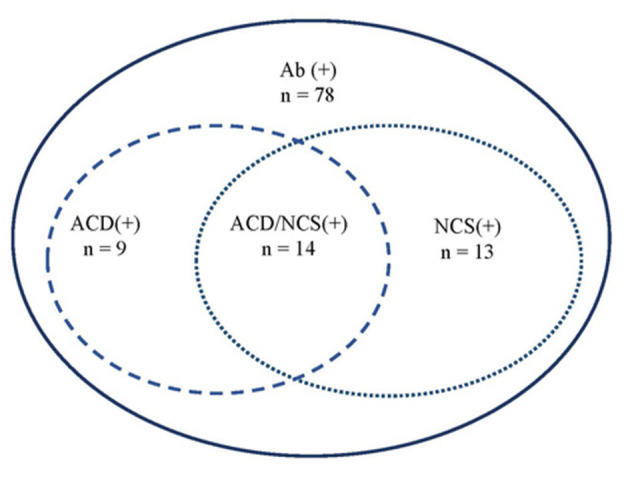
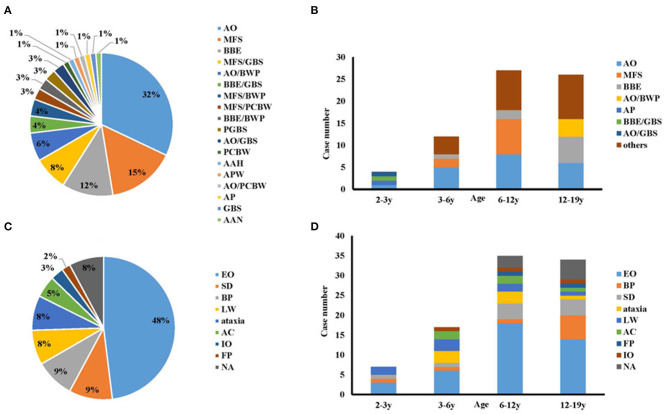
To delineate the comprehensive clinical features of anti-GQ1b antibody syndrome in childhood. The clinical data of children diagnosed with anti-GQ1b antibody syndrome at two Chinese tertiary pediatric neurology centers were collected and analyzed. We also conducted a systematic literature review on anti-GQ1b antibody syndrome in children. This study included 78 children with anti-GQ1b antibody syndrome, consisting of 12 previously unreported cases from the two Chinese centers. The median onset age was 10 years (range, 2-18 years). The most common phenotype was acute ophthalmoparesis (32%), followed by classic Miller Fisher syndrome (15%), and Bickerstaff brainstem encephalitis (12%). External ophthalmoplegia (48%), sensory disturbance (9%), and bulbar palsy (9%) were the three most frequent onset symptom manifestations. Brain or spinal lesions on MRI and abnormal recordings by nerve conduction study were present in 18% (12/68) and 60% (27/45) of cases, respectively. There was CSF albuminocytologic dissociation in 34% of the patients (23/68). IV immunoglobulin alone or combined with steroids or plasma exchange was administered to 58% of patients (42/72). We did not find a significant correlation between early improvement up to 3 months and age onset and phenotype. All patients showed different degrees of recovery, and 81% (57/70) had complete recovery within 1 year. Acute ophthalmoparesis and classic Miller Fisher syndrome are the most common phenotypes of anti-GQ1b antibody syndrome in childhood. The majority of patients show good response to immunotherapy and have favorable prognosis.
为了阐明儿童抗GQ1b抗体综合征的综合临床特征。收集并分析了在中国两家三级儿童神经科中心诊断为抗GQ1b抗体综合征的儿童的临床资料。我们还对儿童抗GQ1b抗体综合征进行了系统的文献综述。本研究纳入了78例抗GQ1b抗体综合征患儿,其中包括来自两家中国中心的12例既往未报道的病例。中位发病年龄为10岁(范围2 - 18岁)。最常见的表型是急性眼肌麻痹(32%),其次是经典的米勒费雪综合征(15%)和巴洛氏脑干脑炎(12%)。眼外肌麻痹(48%)、感觉障碍(9%)和延髓麻痹(9%)是最常见的三种起病症状表现。MRI显示脑或脊髓病变以及神经传导研究记录异常分别见于18%(12/68)和60%(27/45)的病例。34%的患者(23/68)存在脑脊液蛋白细胞分离。58%的患者(42/72)接受了单独静脉注射免疫球蛋白或联合使用类固醇或血浆置换治疗。我们未发现3个月内的早期改善与发病年龄和表型之间存在显著相关性。所有患者均有不同程度的恢复,81%(57/70)在1年内完全恢复。急性眼肌麻痹和经典的米勒费雪综合征是儿童抗GQ1b抗体综合征最常见的表型。大多数患者对免疫治疗反应良好,预后良好。