School of Medicine, University of Dundee, Dundee, UK.
Division of Molecular and Clinical Medicine, University of Dundee, Dundee, UK.
ESC Heart Fail. 2021 Aug;8(4):3168-3179. doi: 10.1002/ehf2.13424. Epub 2021 May 16.
Inflammation is thought to play a role in heart failure (HF) pathophysiology. Neutrophil-to-lymphocyte ratio (NLR) is a simple, routinely available measure of inflammation. Its relationship with other inflammatory biomarkers and its association with clinical outcomes in addition to other risk markers have not been comprehensively evaluated in HF patients.
We evaluated patients with worsening or new-onset HF from the BIOlogy Study to Tailored Treatment in Chronic Heart Failure (BIOSTAT-CHF) study who had available NLR at baseline. The primary outcome was time to all-cause mortality or HF hospitalization. Outcomes were validated in a separate HF population.
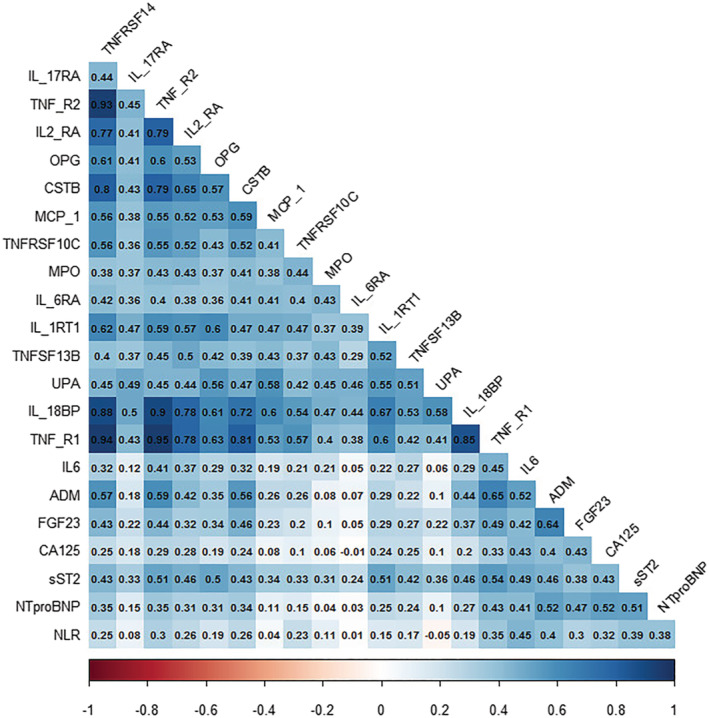
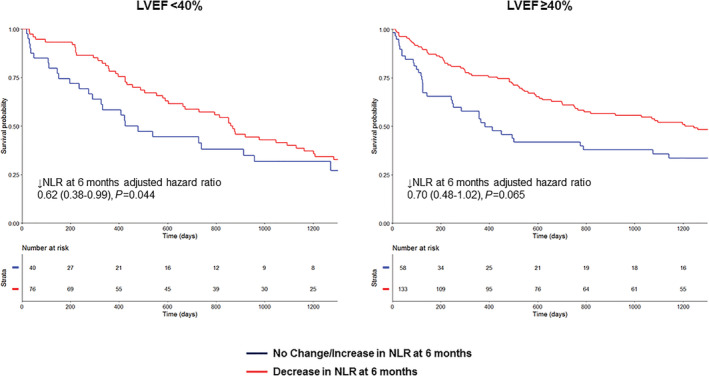
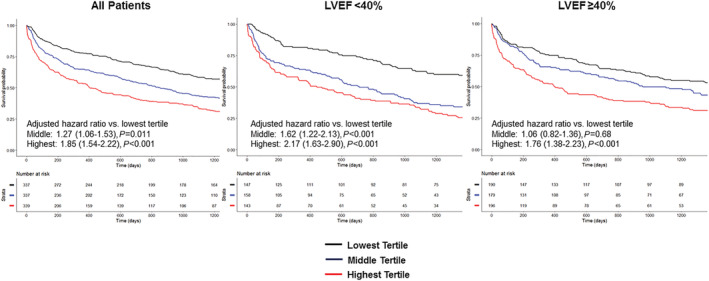
1622 patients were evaluated (including 523 ventricular ejection fraction [LVEF] < 40% and 662 LVEF ≥ 40%). NLR was significantly correlated with biomarkers related to inflammation as well as NT-proBNP. NLR was significantly associated with the primary outcome in patients irrespective of LVEF (hazard ratio [HR] 1.18 per standard deviation increase; 95% confidence interval [CI] 1.11-1.26, P < 0.001). Patients with NLR in the highest tertile had significantly worse outcome than those in the lowest independent of LVEF (<40%: HR 2.75; 95% CI 1.84-4.09, P < 0.001; LVEF ≥ 40%: HR 1.51; 95% CI 1.05-2.16, P = 0.026). When NLR was added to the BIOSTAT-CHF risk score, there were improvements in integrated discrimination index (IDI) and net reclassification index (NRI) for occurrence of the primary outcome (IDI + 0.009; 95% CI 0.00-0.019, P = 0.030; continuous NRI + 0.112, 95% CI 0.012-0.176, P = 0.040). Elevated NLR was similarly associated with adverse outcome in the validation cohort. Decrease in NLR at 6 months was associated with reduced incidence of the primary outcome (HR 0.75; 95% CI 0.57-0.98, P = 0.036).
Elevated NLR is significantly associated with elevated markers of inflammation in HF patients and is associated with worse outcome. Elevated NLR might potentially be useful in identifying high-risk HF patients and may represent a treatment target.
炎症被认为在心力衰竭(HF)发病机制中起作用。中性粒细胞与淋巴细胞比值(NLR)是一种简单的、常规的炎症指标。其与其他炎症生物标志物的关系以及与临床结局的关系(除了其他风险标志物外)在 HF 患者中尚未得到全面评估。
我们评估了 BIOlogy Study to Tailored Treatment in Chronic Heart Failure(BIOSTAT-CHF)研究中基线时可获得 NLR 的恶化或新发 HF 患者。主要结局是全因死亡率或 HF 住院的时间。结局在单独的 HF 人群中得到了验证。
共评估了 1622 例患者(包括 523 例左心室射血分数(LVEF)<40%和 662 例 LVEF≥40%)。NLR 与炎症相关的生物标志物以及 NT-proBNP 呈显著相关。NLR 与无论 LVEF 如何(危险比 [HR] 每标准偏差增加 1.18;95%置信区间 [CI] 1.11-1.26,P<0.001)的主要结局显著相关。NLR 处于最高三分位的患者的结局明显比 NLR 处于最低三分位的患者差,无论 LVEF 如何(<40%:HR 2.75;95%CI 1.84-4.09,P<0.001;LVEF≥40%:HR 1.51;95%CI 1.05-2.16,P=0.026)。当 NLR 被添加到 BIOSTAT-CHF 风险评分中时,对主要结局发生的综合判别指数(IDI)和净重新分类指数(NRI)有所改善(IDI+0.009;95%CI 0.00-0.019,P=0.030;连续 NRI+0.112,95%CI 0.012-0.176,P=0.040)。升高的 NLR 与验证队列中的不良结局也显著相关。6 个月时 NLR 的下降与主要结局发生率的降低相关(HR 0.75;95%CI 0.57-0.98,P=0.036)。
升高的 NLR 与 HF 患者炎症标志物的升高显著相关,并与不良结局相关。升高的 NLR 可能在识别高危 HF 患者方面具有潜在的作用,并且可能是一个治疗靶点。