Colegio de Ciencias de la Salud, Universidad San Francisco de Quito, Quito, Ecuador.
Biodiversity Institute and Department of Ecology & Evolutionary Biology, University of Kansas, Lawrence, Kansas, United States of America.
PLoS One. 2021 May 17;16(5):e0251295. doi: 10.1371/journal.pone.0251295. eCollection 2021.
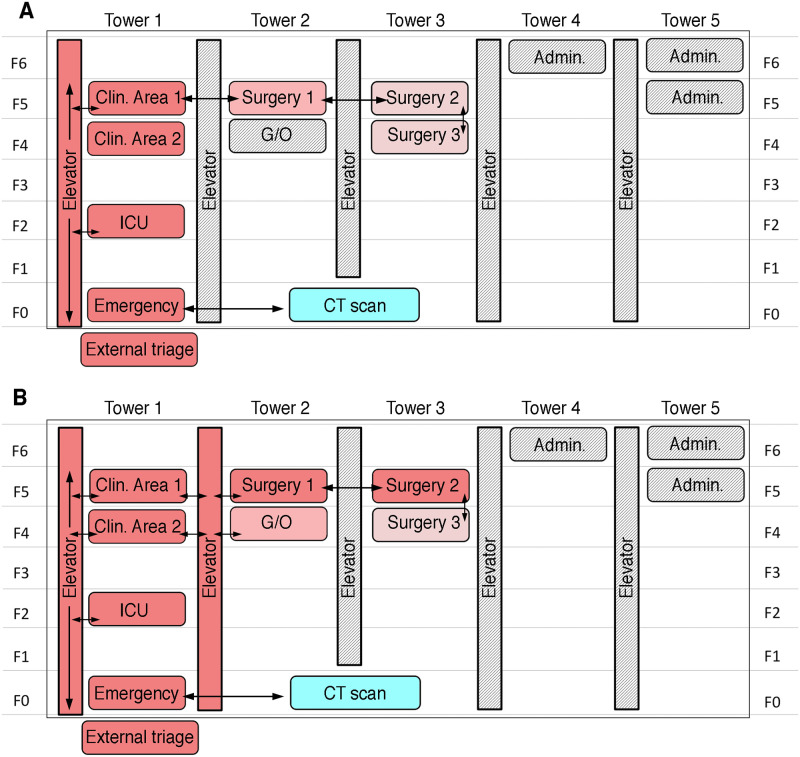
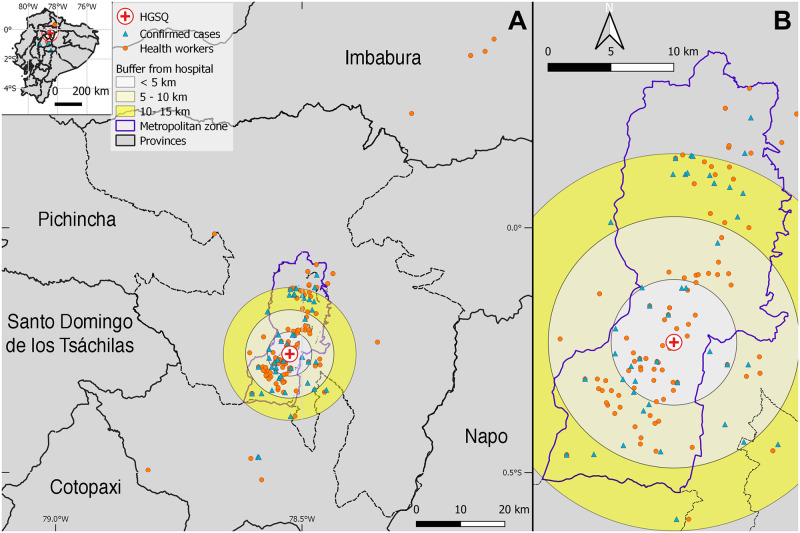
The World Health Organization (WHO) declared coronavirus disease-2019 (COVID-19) a global pandemic on 11 March 2020. In Ecuador, the first case of COVID-19 was recorded on 29 February 2020. Despite efforts to control its spread, SARS-CoV-2 overran the Ecuadorian public health system, which became one of the most affected in Latin America on 24 April 2020. The Hospital General del Sur de Quito (HGSQ) had to transition from a general to a specific COVID-19 health center in a short period of time to fulfill the health demand from patients with respiratory afflictions. Here, we summarized the implementations applied in the HGSQ to become a COVID-19 exclusive hospital, including the rearrangement of hospital rooms and a triage strategy based on a severity score calculated through an artificial intelligence (AI)-assisted chest computed tomography (CT). Moreover, we present clinical, epidemiological, and laboratory data from 75 laboratory tested COVID-19 patients, which represent the first outbreak of Quito city. The majority of patients were male with a median age of 50 years. We found differences in laboratory parameters between intensive care unit (ICU) and non-ICU cases considering C-reactive protein, lactate dehydrogenase, and lymphocytes. Sensitivity and specificity of the AI-assisted chest CT were 21.4% and 66.7%, respectively, when considering a score >70%; regardless, this system became a cornerstone of hospital triage due to the lack of RT-PCR testing and timely results. If health workers act as vectors of SARS-CoV-2 at their domiciles, they can seed outbreaks that might put 1,879,047 people at risk of infection within 15 km around the hospital. Despite our limited sample size, the information presented can be used as a local example that might aid future responses in low and middle-income countries facing respiratory transmitted epidemics.
世界卫生组织(WHO)于 2020 年 3 月 11 日宣布 2019 年冠状病毒病(COVID-19)为全球大流行。在厄瓜多尔,COVID-19 的首例病例于 2020 年 2 月 29 日记录在案。尽管努力控制其传播,但 SARS-CoV-2 还是使厄瓜多尔的公共卫生系统不堪重负,厄瓜多尔于 2020 年 4 月 24 日成为拉丁美洲受影响最严重的国家之一。南部基多综合医院(HGSQ)不得不将其从综合医院转变为专门的 COVID-19 医疗中心,以满足患有呼吸道疾病的患者的健康需求。在这里,我们总结了 HGSQ 为成为 COVID-19 专用医院所采取的措施,包括重新布置医院病房和根据通过人工智能(AI)辅助的胸部计算机断层扫描(CT)计算的严重程度评分进行分诊策略。此外,我们还介绍了 75 例经过实验室检测的 COVID-19 患者的临床,流行病学和实验室数据,这些数据代表了基多市的首例暴发。大多数患者为男性,中位年龄为 50 岁。我们发现,考虑到 C-反应蛋白,乳酸脱氢酶和淋巴细胞,重症监护病房(ICU)和非 ICU 病例的实验室参数存在差异。当考虑得分> 70%时,AI 辅助的胸部 CT 的灵敏度和特异性分别为 21.4%和 66.7%;无论如何,由于缺乏 RT-PCR 测试和及时的结果,该系统成为医院分诊的基石。如果卫生工作者在其家中成为 SARS-CoV-2 的载体,他们可以引发可能使医院周围 15 公里范围内的 1,879,047 人面临感染风险的暴发。尽管我们的样本量有限,但所提供的信息可作为地方示例,可帮助应对未来在面临呼吸道传播性流行病的中低收入国家的疫情。