Yang Kunlin, Cheng Sida, Cai Yukun, Qiao Jiankun, Xu Yangyang, Li Xinfei, Xiong Shengwei, Lu Ye, Mei Aobing, Li Xuesong, Zhou Liqun
Department of Urology, Peking University First Hospital, No. 8 Xishiku St, Xicheng District, Beijing, 100034, China.
Institute of Urology, Peking University, No. 8 Xishiku St, Xicheng District, Beijing, 100034, China.
BMC Womens Health. 2021 May 17;21(1):206. doi: 10.1186/s12905-021-01349-7.
To present the experience with the surgical management of ureteral endometriosis (UE) in our single center.
To present the experience with the surgical management of ureteral endometriosis (UE) in our single center. A retrospective analysis of 40 patients with UE who presented with intraoperative surgical findings of endometriosis involving the ureter and pathology-proven UE was performed.
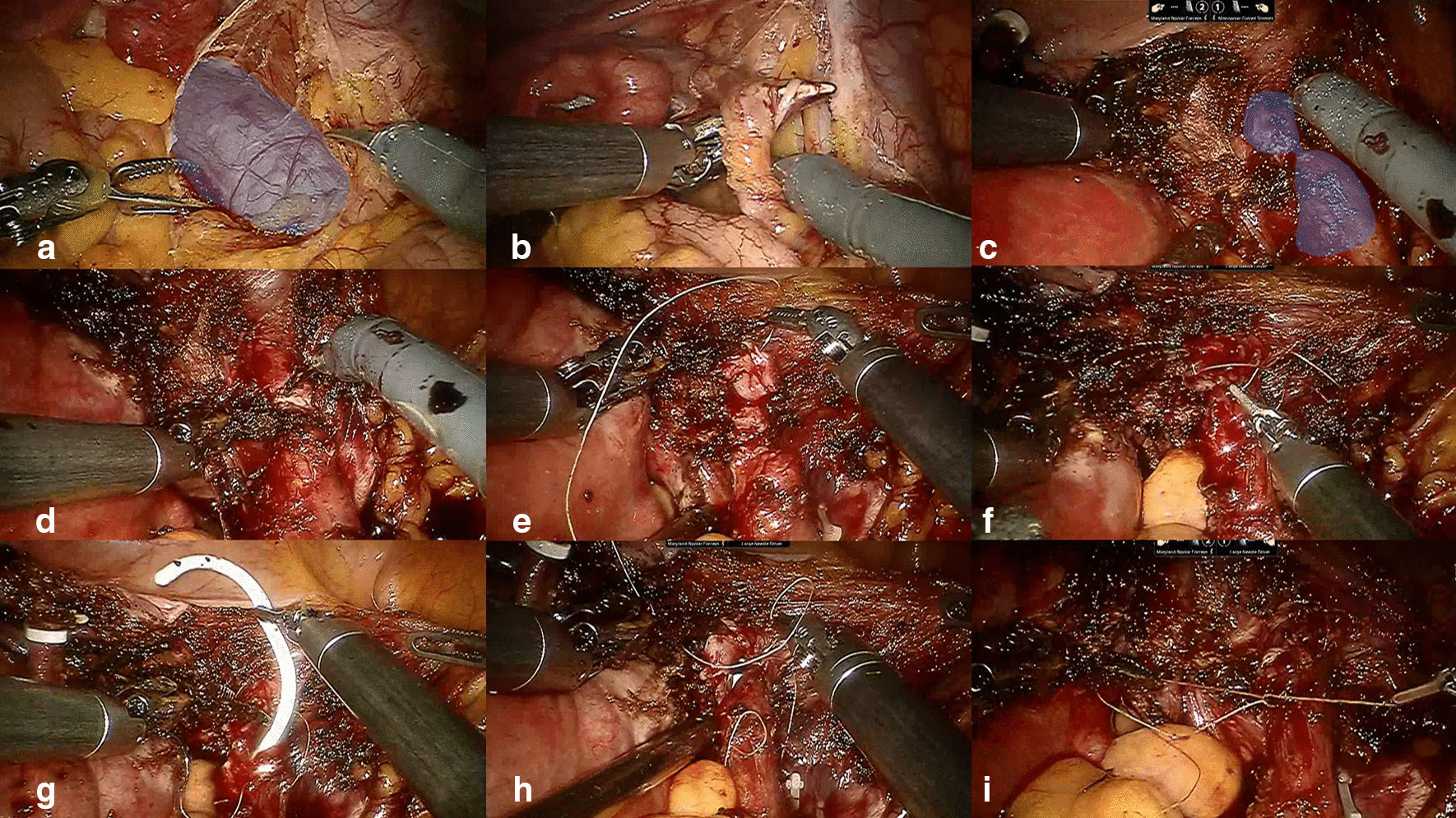
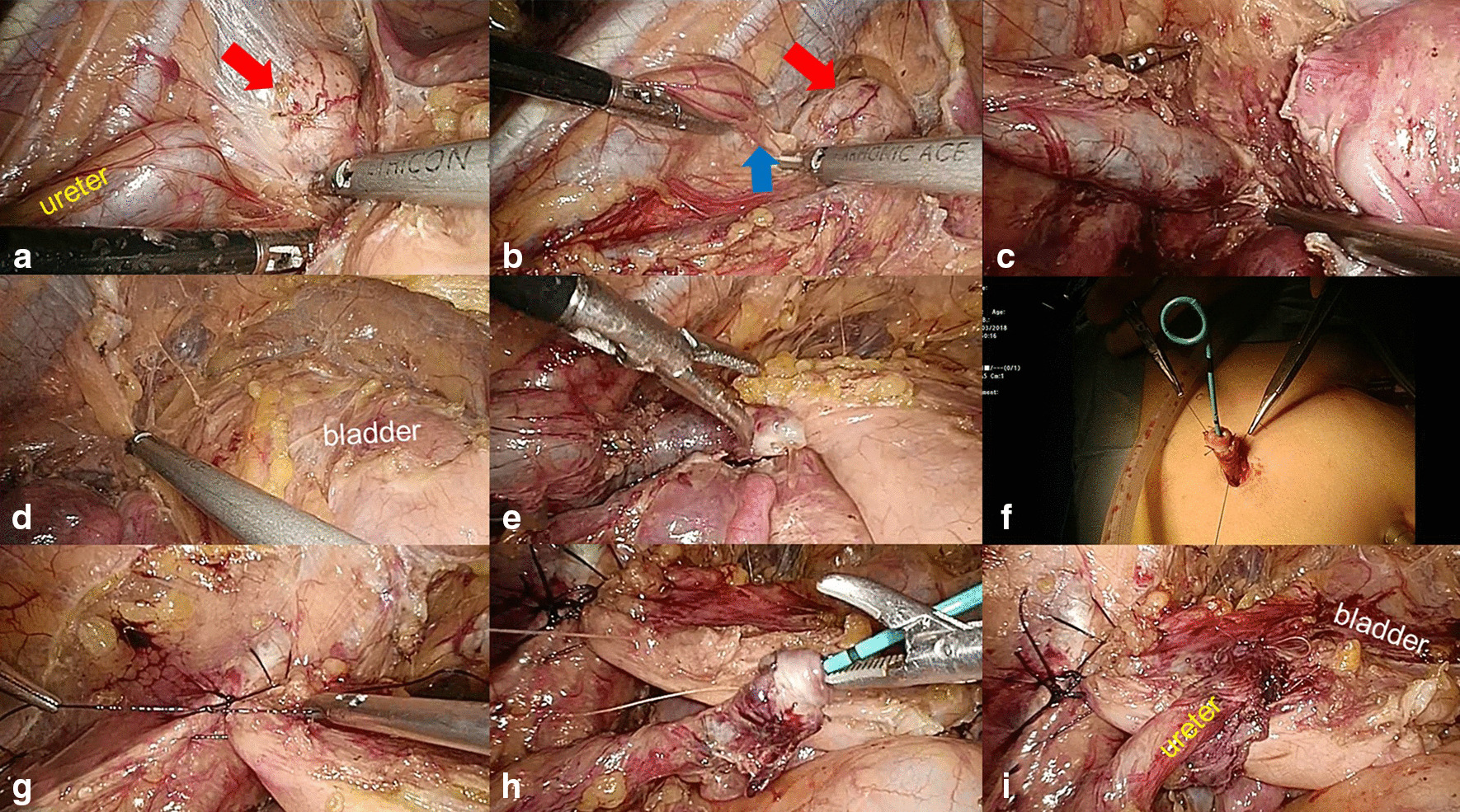
Forty patients (median age, 42.5 years) with histological evidence of UE were included. Six (15%) patients had a history of endometriosis. Twenty-one (52%) patients had urological symptoms, and 19 (48%) patients were asymptomatic. All patients had hydronephrosis. The mean glomerular filtration rate (GFR) of the ipsilateral kidney was significantly worse than that of the contralateral kidney (23.4 vs 54.9 ml/min; P < 0.001). Twelve (30%) patients were treated with ureteroureterostomy (11 open approaches and 1 robotic approach). Twenty-two (55%) patients underwent ureteroneocystostomy (17 open approaches, 4 laparoscopic approaches and 1 robotic approach). Five patients underwent nephroureterectomy. One patient refused aggressive surgery and received ureteroscopic biopsy and ureteral stent placement. Thirteen (33%) patients required gynecological operations. Three (8%) patients in the open group suffered from major surgical complications. Nine (24%) patients received postoperative endocrine therapy. Twenty-eight (70%) patients were followed up (median follow-up time, 71 months). Twenty-four patients received kidney-sparing surgeries. The success rate for these 24 patients was 21/24 (87.5%). The success rates of ureteroneocystostomy and ureteroureterostomy were 15/16 (93.8%) and 5/7 (71.4%), respectively.
Although UE is rare, we should remain vigilant for the disease among female patients with silent hydronephrosis. Typically, a multidisciplinary surgical team is necessary. For patients with severe UE, segmental ureteral resection with ureteroureterostomy (UU) or ureteroneocystostomy may be a preferred choice.
介绍我们单中心输尿管子宫内膜异位症(UE)手术治疗的经验。
介绍我们单中心输尿管子宫内膜异位症(UE)手术治疗的经验。对40例术中发现输尿管有子宫内膜异位且经病理证实为UE的患者进行回顾性分析。
纳入40例有UE组织学证据的患者(中位年龄42.5岁)。6例(15%)患者有子宫内膜异位病史。21例(52%)患者有泌尿系统症状,19例(48%)患者无症状。所有患者均有肾积水。患侧肾脏的平均肾小球滤过率(GFR)明显低于对侧肾脏(23.4 vs 54.9 ml/min;P < 0.001)。12例(30%)患者接受了输尿管输尿管吻合术(11例开放手术和1例机器人手术)。22例(55%)患者接受了输尿管膀胱吻合术(17例开放手术、4例腹腔镜手术和1例机器人手术)。5例患者接受了肾输尿管切除术。1例患者拒绝积极手术,接受了输尿管镜活检和输尿管支架置入术。13例(33%)患者需要妇科手术。开放手术组有3例(8%)患者出现严重手术并发症。9例(24%)患者接受了术后内分泌治疗。28例(70%)患者接受了随访(中位随访时间71个月)。24例患者接受了保留肾脏的手术。这24例患者的成功率为21/24(87.5%)。输尿管膀胱吻合术和输尿管输尿管吻合术的成功率分别为15/16(93.8%)和5/7(71.4%)。
尽管UE罕见,但对于无症状肾积水的女性患者,我们仍应警惕该病。通常,需要一个多学科手术团队。对于严重UE患者,行输尿管节段性切除并输尿管输尿管吻合术(UU)或输尿管膀胱吻合术可能是首选。