Hood Anna M, Strong Heather, Nwankwo Cara, Johnson Yolanda, Peugh James, Mara Constance A, Shook Lisa M, Brinkman William B, Real Francis J, Klein Melissa D, Hackworth Rogelle, Badawy Sherif M, Thompson Alexis A, Raphael Jean L, Yates Amber M, Smith-Whitley Kim, King Allison A, Calhoun Cecelia, Creary Susan E, Piccone Connie M, Hildenbrand Aimee K, Reader Steven K, Neumayr Lynne, Meier Emily R, Sobota Amy E, Rana Sohail, Britto Maria, Saving Kay L, Treadwell Marsha, Quinn Charles T, Ware Russell E, Crosby Lori E
Developmental Neurosciences, Institute of Child Health, University College London, London, United Kingdom.
Behavioral Medicine and Clinical Psychology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States.
JMIR Res Protoc. 2021 May 21;10(5):e27650. doi: 10.2196/27650.
Sickle cell anemia (SCA) is a genetic blood disorder that puts children at a risk of serious medical complications, early morbidity and mortality, and high health care utilization. Until recently, hydroxyurea was the only disease-modifying treatment for this life-threatening disease and has remained the only option for children younger than 5 years. Evidence-based guidelines recommend using a shared decision-making (SDM) approach for offering hydroxyurea to children with SCA (HbSS or HbS/β0 thalassemia) aged as early as 9 months. However, the uptake remains suboptimal, likely because caregivers lack information about hydroxyurea and have concerns about its safety and potential long-term side effects. Moreover, clinicians do not routinely receive training or tools, especially those that provide medical evidence and consider caregivers' preferences and values, to facilitate a shared discussion with caregivers.
The aim of this study is to understand how best to help parents of young children with sickle cell disease and their clinicians have a shared discussion about hydroxyurea (one that considers medical evidence and parent values and preferences).
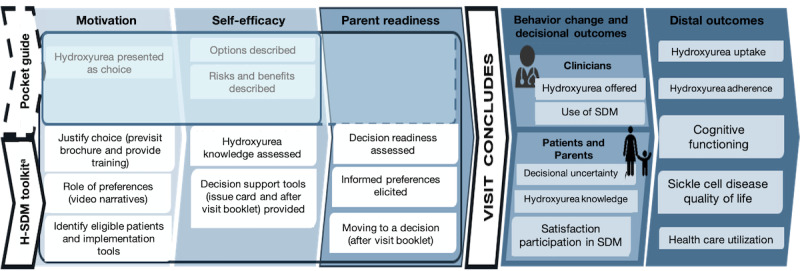
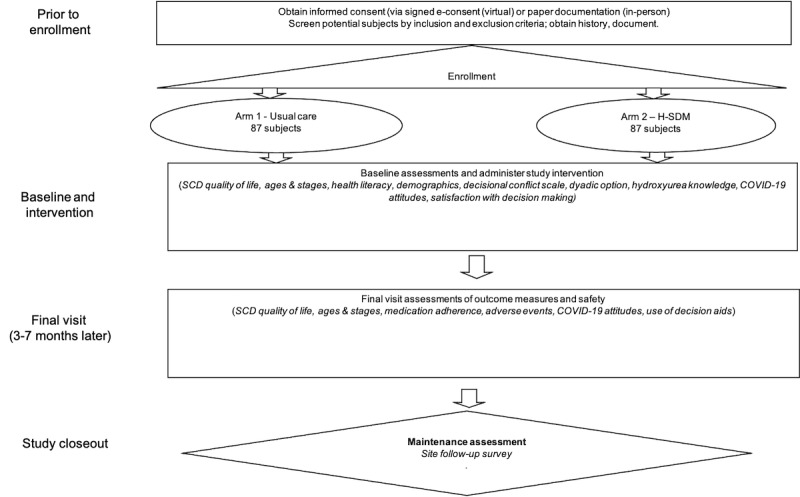
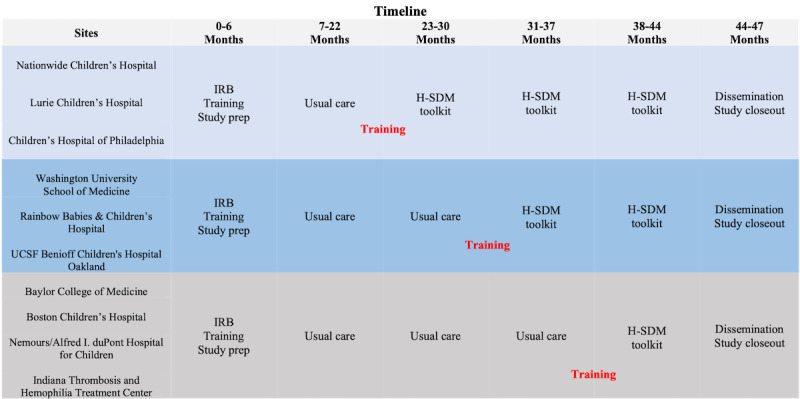
We designed our study to compare the effectiveness of two methods for disseminating hydroxyurea guidelines to facilitate SDM: a clinician pocket guide (ie, usual care) and a clinician hydroxyurea SDM toolkit (H-SDM toolkit). Our primary outcomes are caregiver reports of decisional uncertainty and knowledge of hydroxyurea. The study also assesses the number of children (aged 0-5 years) who were offered and prescribed hydroxyurea and the resultant health outcomes.
The Ethics Committee of the Cincinnati Children's Hospital Medical Center approved this study in November 2017. As of February 2021, we have enrolled 120 caregiver participants.
The long-term objective of this study is to improve the quality of care for children with SCA. Using multicomponent dissemination methods developed in partnership with key stakeholders and designed to address barriers to high-quality care, caregivers of patients with SCA can make informed and shared decisions about their health.
ClinicalTrials.gov NCT03442114; https://clinicaltrials.gov/ct2/show/NCT03442114.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): DERR1-10.2196/27650.
镰状细胞贫血(SCA)是一种遗传性血液疾病,使儿童面临严重医疗并发症、早期发病和死亡以及高医疗保健利用率的风险。直到最近,羟基脲一直是这种危及生命疾病的唯一疾病改善治疗方法,并且仍然是5岁以下儿童的唯一选择。基于证据的指南建议采用共同决策(SDM)方法,尽早为9个月及以上患有SCA(HbSS或HbS/β0地中海贫血)的儿童提供羟基脲。然而,其采用率仍然不理想,可能是因为护理人员缺乏关于羟基脲的信息,并且对其安全性和潜在的长期副作用存在担忧。此外,临床医生通常没有接受培训或获得相关工具,特别是那些提供医学证据并考虑护理人员偏好和价值观的工具,以促进与护理人员的共同讨论。
本研究的目的是了解如何最好地帮助患有镰状细胞病的幼儿的父母及其临床医生就羟基脲进行共同讨论(一种考虑医学证据以及父母价值观和偏好的讨论)。
我们设计本研究以比较两种传播羟基脲指南以促进共同决策的方法的有效性:临床医生袖珍指南(即常规护理)和临床医生羟基脲共同决策工具包(H-SDM工具包)。我们的主要结局是护理人员关于决策不确定性和对羟基脲知识的报告。该研究还评估了接受并开具羟基脲处方的0至5岁儿童的数量以及由此产生的健康结局。
辛辛那提儿童医院医疗中心伦理委员会于2017年11月批准了本研究。截至2021年2月,我们已招募了120名护理人员参与者。
本研究的长期目标是提高SCA儿童的护理质量。通过与关键利益相关者合作开发并旨在解决高质量护理障碍的多组分传播方法,SCA患者的护理人员可以就其健康做出明智的共同决策。
ClinicalTrials.gov NCT03442114;https://clinicaltrials.gov/ct2/show/NCT03442114。
国际注册报告识别码(IRRID):DERR1-10.2196/27650。