Lavoie Jean-Michel, Sridhar Srikala S, Ong Michael, North Scott, Alimohamed Nimira, McLeod Deanna, Eigl Bernhard J
Medical Oncology, BC Cancer - Surrey, Surrey, British Columbia, Canada.
Medical Oncology, Princess Margaret Cancer Center, University of Toronto, Toronto, Ontario, Canada.
Oncologist. 2021 Aug;26(8):e1381-e1394. doi: 10.1002/onco.13827. Epub 2021 Jun 11.
Metastatic urothelial carcinoma (mUC) historically is treated with first-line platinum-based combination chemotherapy, preferably cisplatin plus gemcitabine whenever possible. In recent years, multiple classes of targeted therapy have demonstrated benefit, with some receiving approval in mUC. This review will summarize phase III efficacy and safety data for targeted agents, principally immune checkpoint inhibitors (ICIs), as either first-line or first-line switch-maintenance therapy for mUC and interpret these findings in the context of the current treatment landscape.
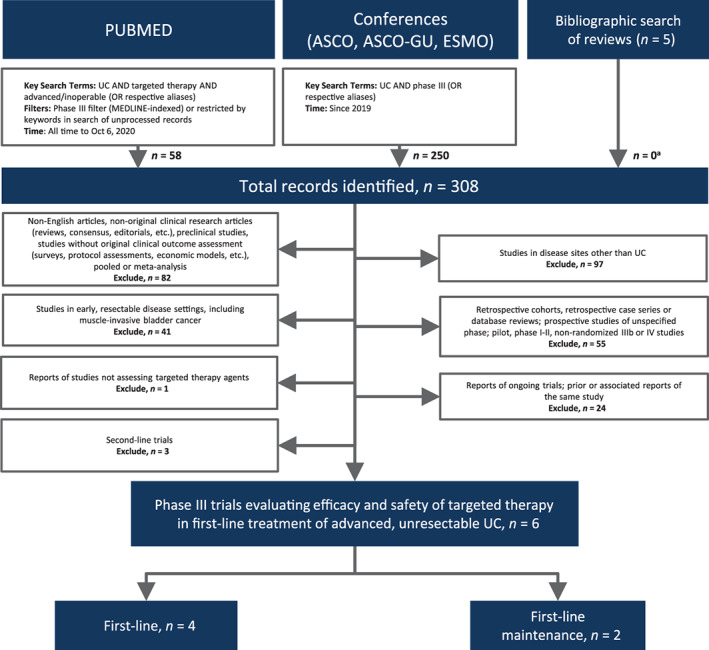
Published and presented phase III data on targeted therapy for the first-line or first-line switch-maintenance treatment of mUC were identified using the key search terms "targeted therapy" AND "urothelial carcinoma" AND "advanced" OR respective aliases according to the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Of the six eligible phase III targeted therapy trials, two assessing ICIs met their primary endpoints in platinum-eligible patients. First-line ICI plus chemotherapy combinations have not improved overall survival (OS), although final OS results of the IMVigor 130 trial are pending. Switch-maintenance using an ICI in patients achieving at least stable disease following platinum-based chemotherapy statistically significantly improved OS (21.4 vs. 14.3 months, hazard ratio, 0.69; 95% confidence interval, 0.56-0.86; p = .001). Current sequencing options for mUC include first-line platinum-based chemotherapy with a switch to ICI either immediately or upon disease progression.
Recent targeted therapy trials have expanded ICI sequencing options for mUC. The treatment landscape is likely to evolve rapidly, with results from multiple phase III trials expected in the next 5 years.
Multiple classes of targeted agents are approved for use in metastatic urothelial carcinoma (mUC). Six phase III trials have recently provided insight on the benefit of these agents in the first-line setting. In platinum-eligible patients, immune checkpoint inhibitors (ICIs) combined with first-line platinum-based chemotherapy failed to demonstrate improved survival, although ICI monotherapy as switch-maintenance significantly improved overall survival in patients with mUC who had achieved at least stable disease following first-line platinum-based chemotherapy. In patients ineligible for any chemotherapy, pembrolizumab, atezolizumab, or pembrolizumab in combination with enfortumab vedotin may be options.
转移性尿路上皮癌(mUC)历来采用一线铂类联合化疗,只要有可能,首选顺铂加吉西他滨。近年来,多种靶向治疗已显示出疗效,其中一些已在mUC中获得批准。本综述将总结靶向药物(主要是免疫检查点抑制剂[ICI])作为mUC一线或一线转换维持治疗的III期疗效和安全性数据,并在当前治疗格局的背景下解读这些发现。
根据系统评价和Meta分析的首选报告项目(PRISMA)指南,使用关键检索词“靶向治疗”、“尿路上皮癌”、“晚期”或各自的别名,识别已发表和已展示的关于mUC一线或一线转换维持治疗的靶向治疗III期数据。
在六项符合条件的III期靶向治疗试验中,两项评估ICI的试验在适合铂类治疗的患者中达到了主要终点。一线ICI加化疗联合方案并未改善总生存期(OS),尽管IMVigor 130试验的最终OS结果尚未得出。在铂类化疗后至少病情稳定的患者中,使用ICI进行转换维持治疗在统计学上显著改善了OS(21.4个月对14.3个月,风险比为0.69;95%置信区间为0.56 - 0.86;p = 0.001)。mUC目前的序贯治疗选择包括一线铂类化疗,可立即或在疾病进展时转换为ICI。
近期的靶向治疗试验扩大了mUC的ICI序贯治疗选择。治疗格局可能会迅速演变,预计未来5年内将有多项III期试验的结果。
多种靶向药物已被批准用于转移性尿路上皮癌(mUC)。六项III期试验最近提供了这些药物在一线治疗中的疗效见解。在适合铂类治疗的患者中,免疫检查点抑制剂(ICI)与一线铂类化疗联合使用未能显示出生存改善,尽管ICI单药作为转换维持治疗显著改善了在一线铂类化疗后至少病情稳定的mUC患者的总生存期。在不适合任何化疗的患者中,帕博利珠单抗、阿替利珠单抗或帕博利珠单抗与恩杂鲁胺联合使用可能是选择。