Department of Pharmaceutical and Health Economics, School of Pharmacy, University of Southern California, 635 Downey Way, Verna & Peter Dauterive Hall, VPD 312, Los Angeles, CA, 90089-3333, USA.
Center for Biomedical Innovation, Massachusetts Institute of Technology, Cambridge, MA, USA.
Sci Rep. 2021 May 25;11(1):10838. doi: 10.1038/s41598-021-90405-1.
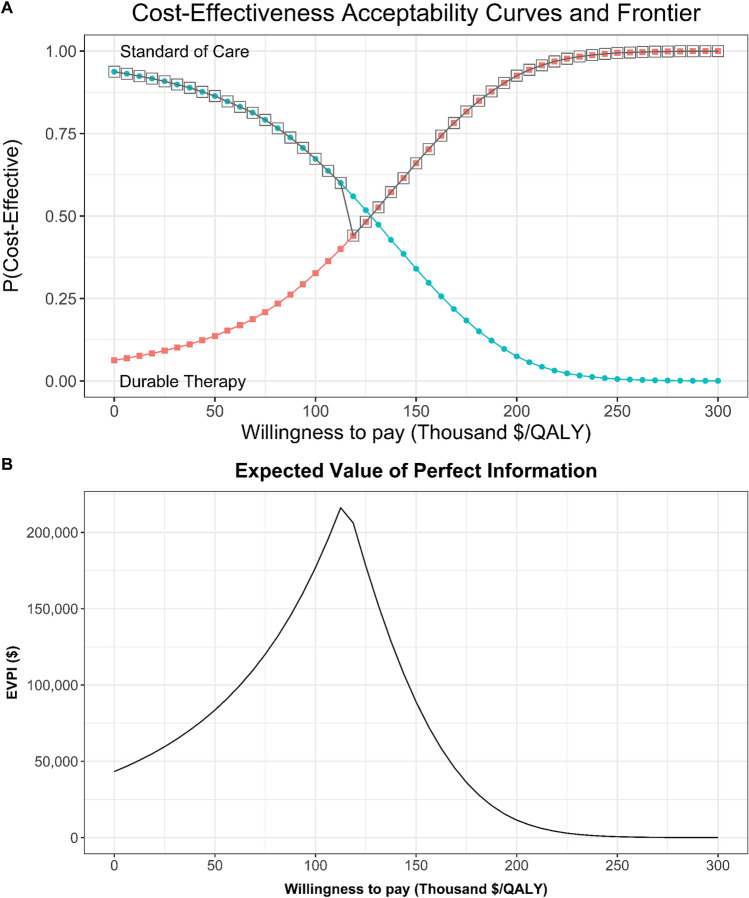
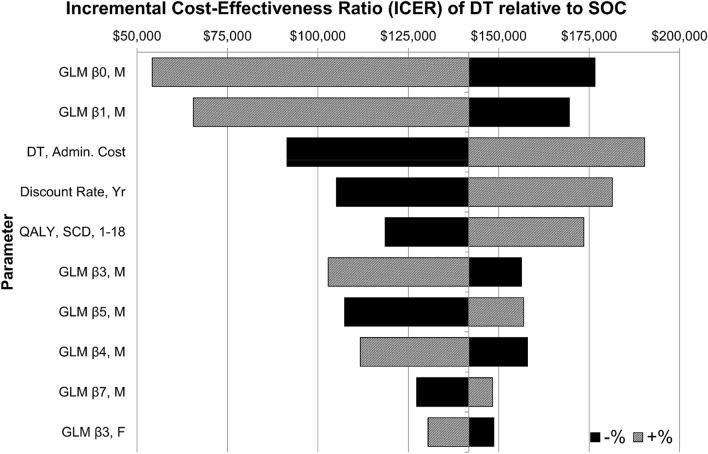
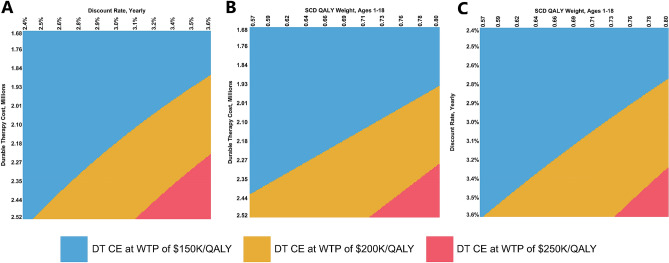
Sickle cell disease (SCD) is a group of inherited genetic conditions associated with lifelong complications and increased healthcare resource utilization. Standard treatment for SCD in the US varies based on stage of the disease and observed clinical severity. In this study, we aim to evaluate the potential cost-effectiveness of a durable cell or gene therapy cure for sickle cell disease from the US healthcare sector perspective. We developed a lifetime Markov model to evaluate the cost-effectiveness of a hypothetical single-administration durable treatment (DT) for SCD provided at birth, relative to standard of care (SOC). We informed model inputs including direct healthcare costs, health state utility weights, transition probabilities, and mortality rates using a retrospective database analysis of commercially insured individuals and the medical literature. Our primary outcome of interest was the incremental cost-effectiveness ratio (ICER) of DT versus SOC evaluated at a base case willingness-to-pay (WTP) threshold of $150,000 per quality-adjusted life year (QALY). We tested the robustness of our base case findings through scenario, deterministic sensitivity (DSA), and probabilistic sensitivity analyses (PSA). In the base case analysis, treatment with DT was cost-effective with an ICER of $140,877/QALY relative to SOC for a hypothetical cohort involving 47% females. Both males (ICER of $135,574/QALY) and females (ICER of $146,511/QALY) were similarly cost-effective to treat. In univariate DSA the base case ICER was most sensitive to the costs of treating males, DT treatment cost, and the discount rate. In PSA, DT was cost-effective in 32.7%, 66.0%, and 92.6% of 10,000 simulations at WTP values of $100,000, $150,000, and $200,000 per QALY, respectively. A scenario analysis showed cost-effectiveness of DT is highly contingent on assumed lifetime durability of the cure. A hypothetical cell or gene therapy cure for SCD is likely to be cost-effective from the US healthcare sector perspective. Large upfront costs of a single administration cure are offset by significant downstream gains in health for patients treated early in life. We find cost-effectiveness outcomes do not vary substantially by gender; however, several model parameters including assumed durability and upfront cost of DT are likely to influence cost-effectiveness findings.
镰状细胞病 (SCD) 是一组与终生并发症和增加医疗资源利用相关的遗传性疾病。美国 SCD 的标准治疗因疾病阶段和观察到的临床严重程度而异。在这项研究中,我们旨在从美国医疗保健部门的角度评估镰状细胞病的持久细胞或基因治疗的潜在成本效益。我们开发了一个终生马尔可夫模型,以评估假设的单次持久治疗 (DT) 对 SCD 的成本效益,该治疗在出生时提供,与标准护理 (SOC) 相比。我们使用商业保险个人和医学文献的回顾性数据库分析来告知模型输入,包括直接医疗成本、健康状态效用权重、转移概率和死亡率。我们的主要研究结果是 DT 与 SOC 相比的增量成本效益比 (ICER),在一个 150,000 美元/QALY 的意愿支付 (WTP) 阈值下进行评估。我们通过情景、确定性敏感性 (DSA) 和概率敏感性分析 (PSA) 测试了我们基本案例结果的稳健性。在基本案例分析中,与 SOC 相比,假设涉及 47%女性的队列中,DT 的治疗具有成本效益,ICER 为 140,877/QALY。男性(ICER 为 135,574/QALY)和女性(ICER 为 146,511/QALY)同样具有成本效益。在单变量 DSA 中,基本案例 ICER 对男性治疗成本、DT 治疗成本和贴现率最为敏感。在 PSA 中,在 WTP 值为 100,000 美元、150,000 美元和 200,000 美元/QALY 的 10,000 次模拟中,DT 分别在 32.7%、66.0%和 92.6%的模拟中具有成本效益。一个方案分析表明,DT 的成本效益高度依赖于假设的治疗终身耐久性。从美国医疗保健部门的角度来看,镰状细胞病的假设细胞或基因治疗可能具有成本效益。单次给药治疗的前期巨额成本被患者在生命早期接受治疗后在健康方面的显著收益所抵消。我们发现,成本效益结果在性别方面没有显著差异;然而,包括假设的耐久性和 DT 的前期成本在内的几个模型参数可能会影响成本效益结果。