McCoach Caroline E, Yu Aiming, Gandara David R, Riess Jonathan W, Vang Daniel P, Li Tiahong, Lara Primo N, Gubens Matthew, Lara Frances, Mack Philip C, Beckett Laurel A, Kelly Karen
Helen Diller Family Comprehensive Cancer Center, University of California, San Francisco, CA.
University of California Davis Comprehensive Cancer Center, Sacramento, CA.
JCO Precis Oncol. 2021 Jan 14;1. doi: 10.1200/PO.20.00279. eCollection 2021.
MET dysregulation is an oncogenic driver in non-small-cell lung cancer (NSCLC), as well as a mechanism of TKI (tyrosine kinase inhibitor) resistance in patients with epidermal growth factor receptor ()-mutated disease. This study was conducted to determine safety and preliminary efficacy of the combination EGFR and MET inhibitors as a strategy to overcome and/or delay EGFR-TKI resistance.
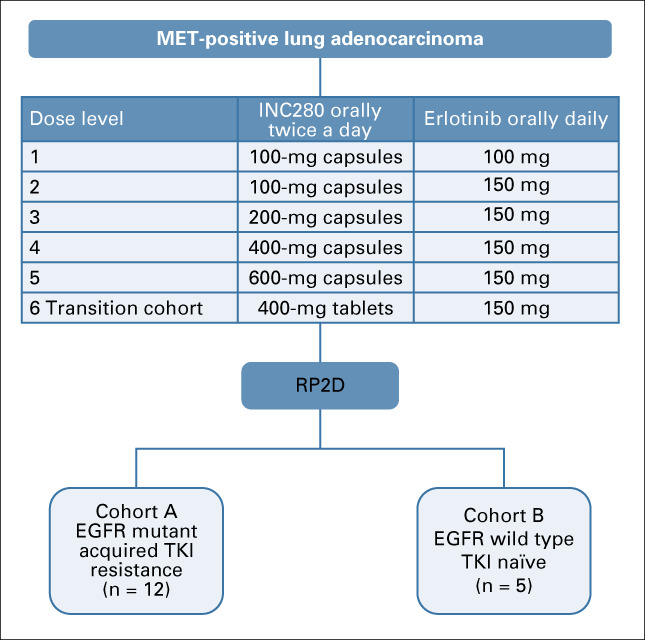
A standard 3 + 3 dose-escalation trial of capmatinib in combination with erlotinib in patients with MET-positive NSCLC was used. Eighteen patients in the dose-escalation cohort received 100-600 mg twice daily of capmatinib with 100-150 mg daily of erlotinib. There were two dose-expansion cohorts. Cohort A included 12 patients with -mutant tumors resistant to TKIs. Cohort B included five patients with wild-type tumors. The primary outcome was to assess safety and determine the recommended phase II dose (RP2D) of the combination.
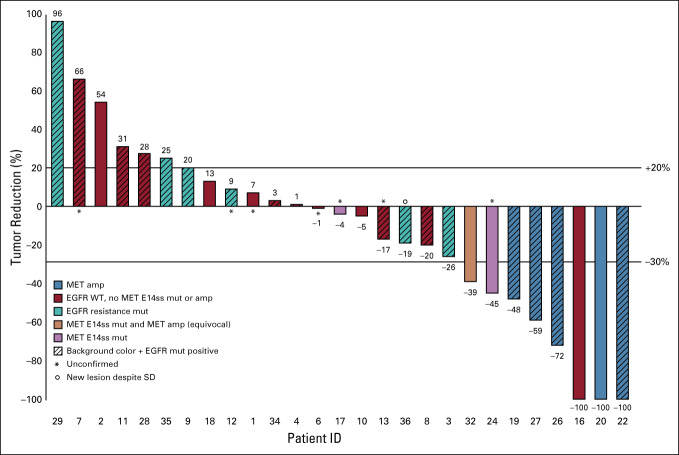
The most common adverse events of any grade were rash (62.9%), fatigue (51%), and nausea (45.7%). Capmatinib exhibited nonlinear pharmacokinetics combined with erlotinib, while showing no significant drug interactions. The RP2D was 400 mg twice daily capmatinib tablets with 150 mg daily erlotinib. The overall response rate (ORR) and DCR in dose-expansion cohort A was 50% and 50%, respectively. In cohort B, the ORR and disease control rate were 75% and 75%.
Capmatinib in combination with erlotinib demonstrated safety profiles consistent with prior studies. We observed efficacy in specific patient populations. Continued evaluation of capmatinib plus EGFR-TKIs is warranted in patients with activating mutations.
MET失调是非小细胞肺癌(NSCLC)的致癌驱动因素,也是表皮生长因子受体(EGFR)突变患者对酪氨酸激酶抑制剂(TKI)耐药的机制。本研究旨在确定联合使用EGFR和MET抑制剂作为克服和/或延缓EGFR-TKI耐药策略的安全性和初步疗效。
采用卡马替尼联合厄洛替尼治疗MET阳性NSCLC患者的标准3+3剂量递增试验。剂量递增队列中的18名患者接受每日两次100-600mg的卡马替尼和每日100-150mg的厄洛替尼。有两个剂量扩展队列。队列A包括12名对TKI耐药的EGFR突变肿瘤患者。队列B包括5名EGFR野生型肿瘤患者。主要结局是评估安全性并确定联合用药的推荐II期剂量(RP2D)。
任何级别的最常见不良事件为皮疹(62.9%)、疲劳(51%)和恶心(45.7%)。卡马替尼与厄洛替尼联合时表现出非线性药代动力学,同时未显示出明显的药物相互作用。RP2D为每日两次400mg卡马替尼片加每日150mg厄洛替尼。剂量扩展队列A中的总缓解率(ORR)和疾病控制率(DCR)分别为50%和50%。在队列B中,ORR和疾病控制率分别为75%和75%。
卡马替尼联合厄洛替尼显示出与先前研究一致的安全性。我们在特定患者群体中观察到了疗效。对于有EGFR激活突变的患者,有必要继续评估卡马替尼加EGFR-TKIs的疗效。