Department of Radiotherapy, Erasmus MC Cancer Institute, University Medical Center Rotterdam, Rotterdam, Zuid Holland, 3015GD, The Netherlands.
Med Phys. 2021 Aug;48(8):4139-4147. doi: 10.1002/mp.14993. Epub 2021 Jun 28.
To propose and validate a fully automated multicriterial treatment planning solution for a CyberKnife® equipped with an InCise 2 multileaf collimator.
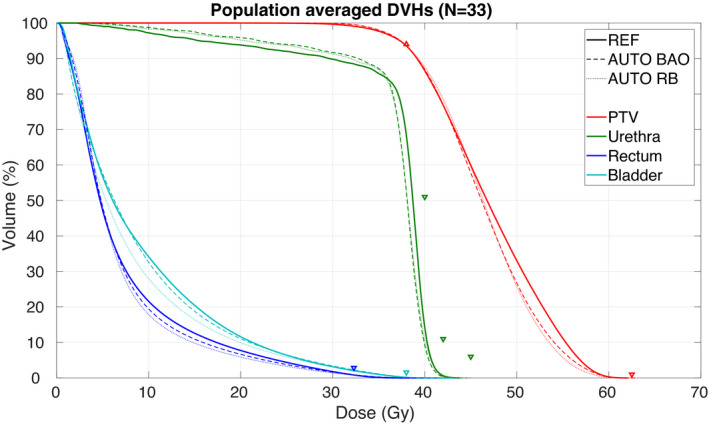
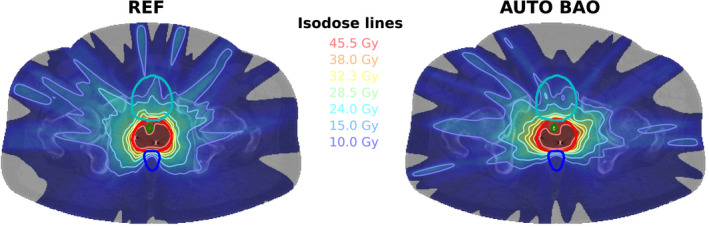
The AUTO BAO plans are generated using fully automated prioritized multicriterial optimization (AUTO MCO) of pencil-beam fluence maps with integrated noncoplanar beam angle optimization (BAO), followed by MLC segment generation. Both the AUTO MCO and segmentation algorithms have been developed in-house. AUTO MCO generates for each patient a single, high-quality Pareto-optimal IMRT plan. The segmentation algorithm then accurately mimics the AUTO MCO 3D dose distribution, while considering all candidate beams simultaneously, rather than replicating the fluence maps. Pencil-beams, segment dose depositions, and final dose calculations are performed with a stand-alone version of the clinical dose calculation engine. For validation, AUTO BAO plans were generated for 33 prostate SBRT patients and compared to reference plans (REF) that were manually generated with the commercial treatment planning system (TPS), in absence of time pressure. REF plans were also compared to AUTO RB plans, for which fluence map optimization was performed for the beam angle configuration used in the REF plan, and the segmentation could use all these beams or only a subset, depending on the dosimetry.
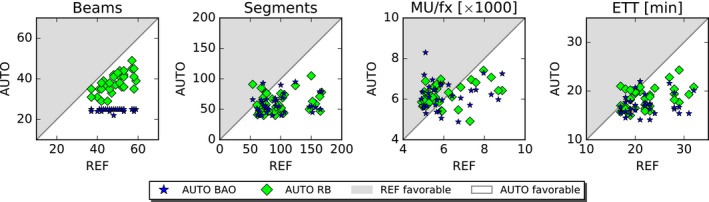
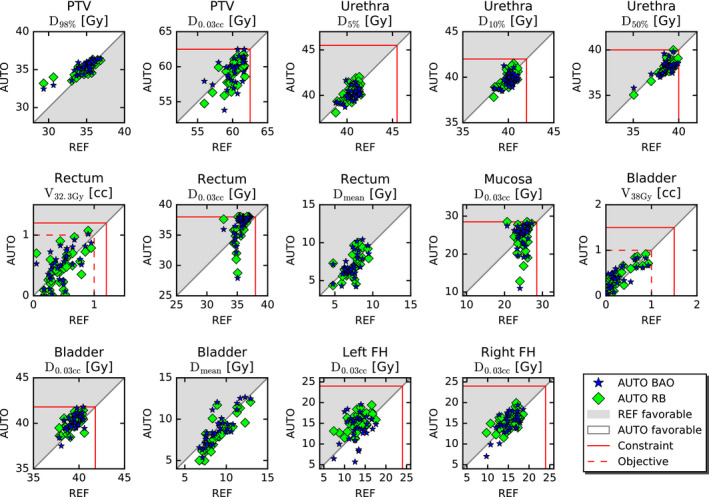
AUTO BAO plans were clinically acceptable and dosimetrically similar to REF plans, but had on average reduced numbers of beams ((beams in AUTO BAO)/(beams in REF) (relative improvement): 24.7/48.3 (-49%)), segments (59.5/98.9 (-40%)), and delivery times (17.1/22.3 min. (-23%)). Dosimetry of AUTO RB and REF were also similar, but AUTO RB used on average fewer beams (38.0/48.3 (-21%)) and had on average shorter delivery times (18.6/22.3 min. (-17%)). Delivered Monitor Units (MU) were similar for all three planning approaches.
A new, vendor-independent optimization workflow for fully automated generation of deliverable high-quality CyberKnife® plans was proposed, including BAO. Compared to manual planning with the commercial TPS, fraction delivery times were reduced by 5.3 min. (-23%) due to large reductions in beam and segment numbers.
提出并验证一种用于配备 InCise 2 多叶准直器的 CyberKnife®的全自动多标准治疗计划解决方案。
AUTO BAO 计划是通过对铅笔束通量图进行全自动优先级多标准优化(AUTO MCO)并结合非共面射束角度优化(BAO)生成的,然后生成 MLC 段。AUTO MCO 和分割算法均为内部开发。AUTO MCO 为每个患者生成一个单一的高质量 Pareto 最优的调强放疗计划。然后,分割算法准确地模拟 AUTO MCO 的 3D 剂量分布,同时同时考虑所有候选射束,而不是复制通量图。铅笔束、段剂量沉积和最终剂量计算使用临床剂量计算引擎的独立版本进行。为了验证,为 33 例前列腺 SBRT 患者生成了 AUTO BAO 计划,并与在没有时间压力的情况下手动生成的参考计划(REF)进行了比较。REF 计划还与 AUTO RB 计划进行了比较,对于 REF 计划使用的射束角度配置进行了通量图优化,并且分割可以使用所有这些射束或仅使用子集,具体取决于剂量学。
AUTO BAO 计划在临床上是可以接受的,与 REF 计划在剂量学上相似,但平均减少了射束数量((AUTO BAO 中的射束数)/(REF 中的射束数)(相对改善):24.7/48.3(-49%))、段数(59.5/98.9(-40%))和输送时间(17.1/22.3 分钟。(-23%))。AUTO RB 和 REF 的剂量学也相似,但 AUTO RB 平均使用的射束较少(38.0/48.3(-21%)),平均输送时间较短(18.6/22.3 分钟。(-17%))。所有三种计划方法的输送的监视器单位(MU)相似。
提出了一种新的、与供应商无关的全自动生成可交付的高质量 CyberKnife®计划的优化工作流程,包括 BAO。与使用商业 TPS 进行手动规划相比,由于射束和段数的大量减少,分次输送时间减少了 5.3 分钟。(-23%)。