CHU de Lille, Médecine Intensive Réanimation, Lille, France.
INSERM U1285, Université de Lille, CNRS, UMR 8576, Unité de Glycobiologie Structurale et Fonctionnelle, Lille, France.
Am J Respir Crit Care Med. 2021 Sep 1;204(5):546-556. doi: 10.1164/rccm.202101-0030OC.
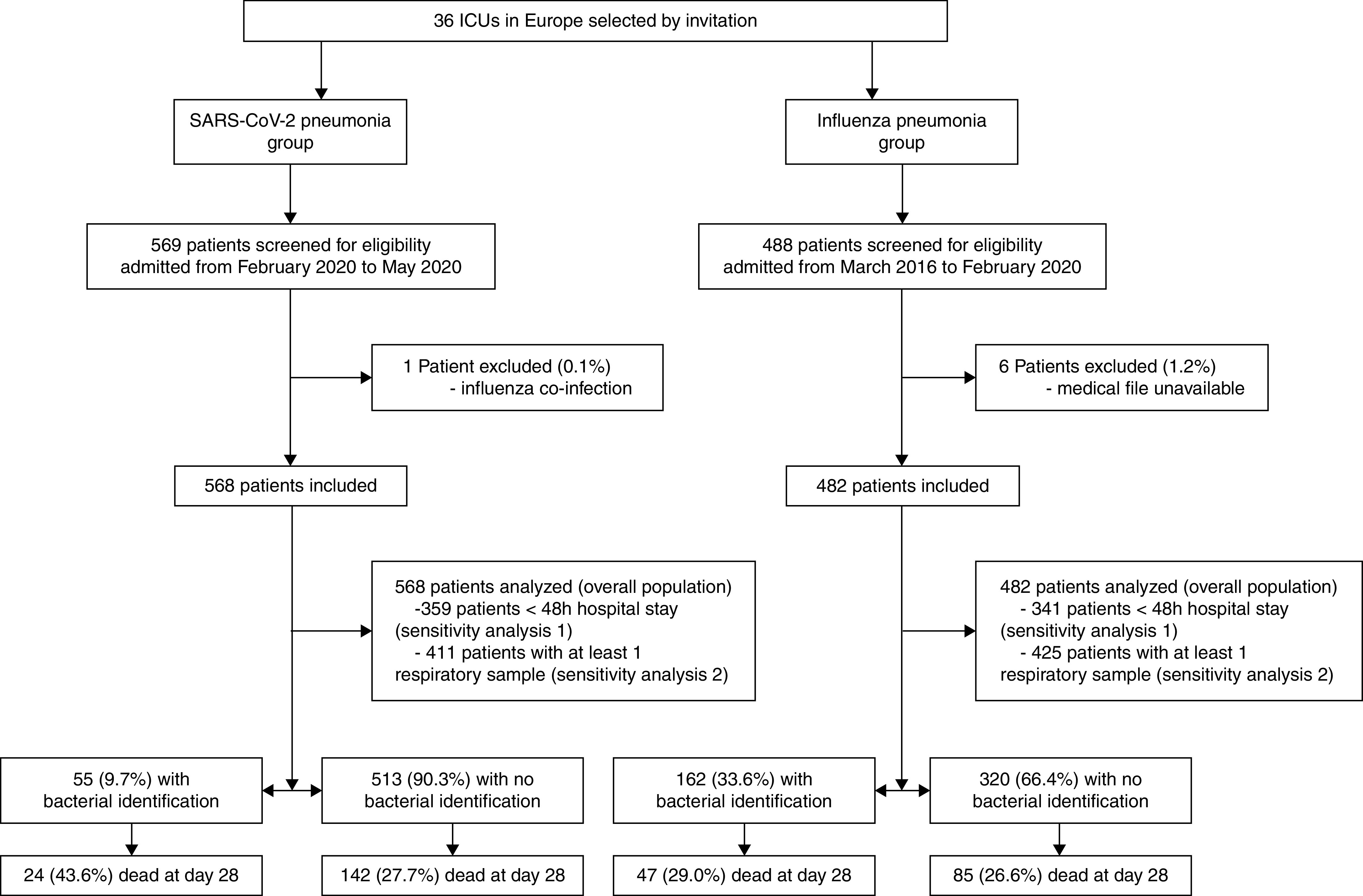
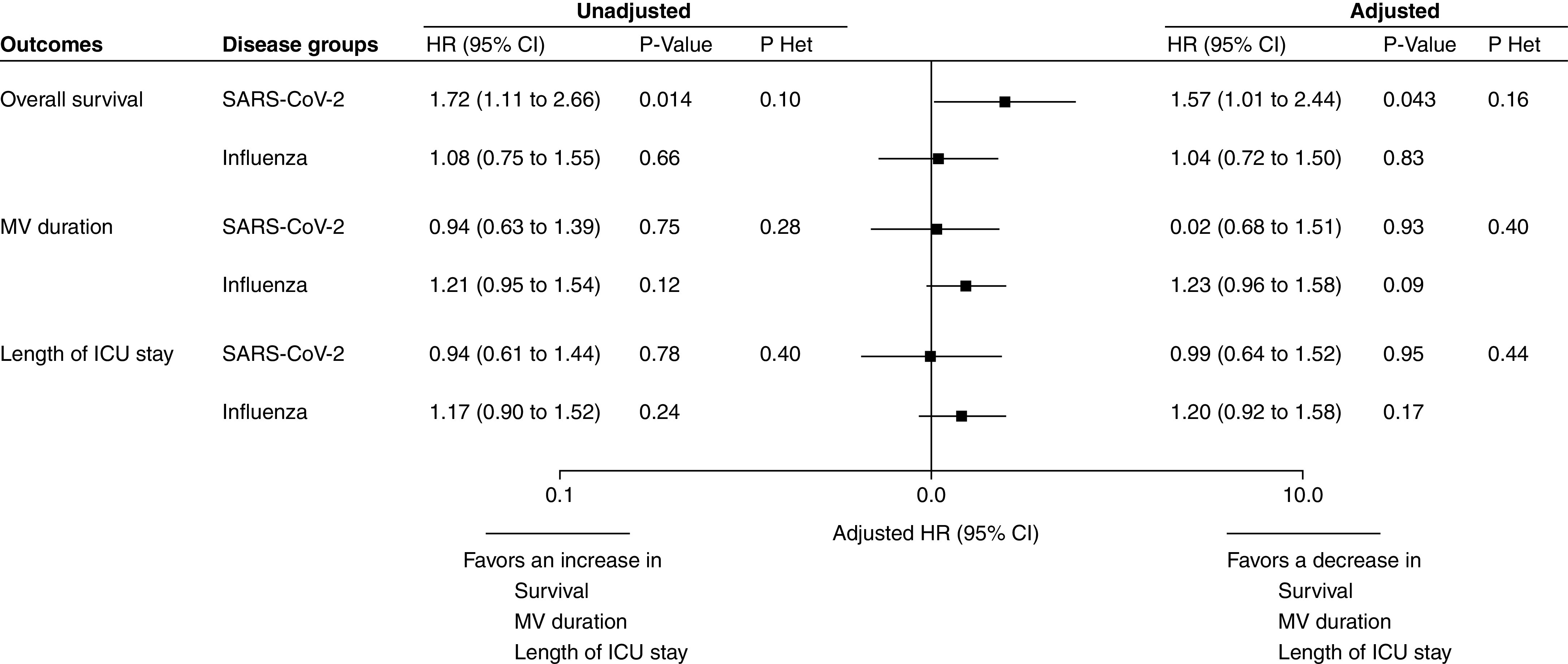
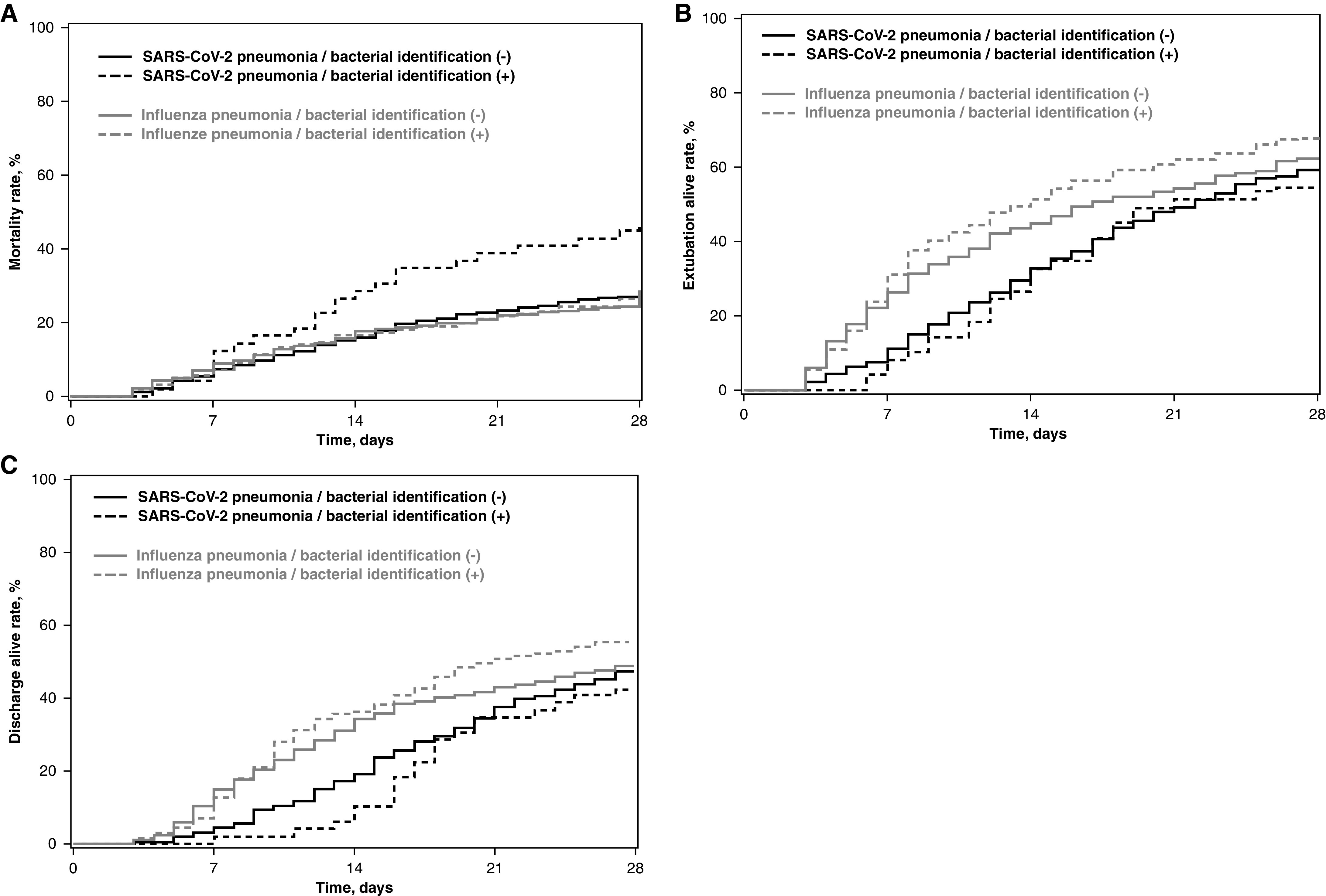
Early empirical antimicrobial treatment is frequently prescribed to critically ill patients with coronavirus disease (COVID-19) based on Surviving Sepsis Campaign guidelines. We aimed to determine the prevalence of early bacterial identification in intubated patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia, as compared with influenza pneumonia, and to characterize its microbiology and impact on outcomes. A multicenter retrospective European cohort was performed in 36 ICUs. All adult patients receiving invasive mechanical ventilation >48 hours were eligible if they had SARS-CoV-2 or influenza pneumonia at ICU admission. Bacterial identification was defined by a positive bacterial culture within 48 hours after intubation in endotracheal aspirates, BAL, blood cultures, or a positive pneumococcal or legionella urinary antigen test. A total of 1,050 patients were included (568 in SARS-CoV-2 and 482 in influenza groups). The prevalence of bacterial identification was significantly lower in patients with SARS-CoV-2 pneumonia compared with patients with influenza pneumonia (9.7 vs. 33.6%; unadjusted odds ratio, 0.21; 95% confidence interval [CI], 0.15-0.30; adjusted odds ratio, 0.23; 95% CI, 0.16-0.33; < 0.0001). Gram-positive cocci were responsible for 58% and 72% of coinfection in patients with SARS-CoV-2 and influenza pneumonia, respectively. Bacterial identification was associated with increased adjusted hazard ratio for 28-day mortality in patients with SARS-CoV-2 pneumonia (1.57; 95% CI, 1.01-2.44; = 0.043). However, no significant difference was found in the heterogeneity of outcomes related to bacterial identification between the two study groups, suggesting that the impact of coinfection on mortality was not different between patients with SARS-CoV-2 and influenza. Bacterial identification within 48 hours after intubation is significantly less frequent in patients with SARS-CoV-2 pneumonia than patients with influenza pneumonia.Clinical trial registered with www.clinicaltrials.gov (NCT04359693).
早期经验性抗菌治疗常根据拯救脓毒症运动指南,用于治疗患有冠状病毒病(COVID-19)的危重症患者。我们旨在确定与流感性肺炎相比,严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)肺炎患者中早期细菌鉴定的流行率,并对其微生物学和对结局的影响进行特征描述。在 36 个 ICU 中进行了一项多中心回顾性欧洲队列研究。如果在 ICU 入院时患有 SARS-CoV-2 或流感性肺炎,且接受>48 小时有创机械通气的所有成年患者均符合纳入条件。通过在气管内吸出物、BAL、血培养物中培养出阳性细菌,或通过阳性肺炎球菌或军团菌尿抗原试验来定义细菌鉴定。共纳入 1050 例患者(SARS-CoV-2 组 568 例,流感组 482 例)。与流感性肺炎患者相比,SARS-CoV-2 肺炎患者的细菌鉴定率显著较低(9.7% vs. 33.6%;未调整优势比,0.21;95%置信区间[CI],0.15-0.30;调整优势比,0.23;95%CI,0.16-0.33;<0.0001)。革兰阳性球菌分别占 SARS-CoV-2 和流感性肺炎患者合并感染的 58%和 72%。细菌鉴定与 SARS-CoV-2 肺炎患者 28 天死亡率的调整后危险比增加相关(1.57;95%CI,1.01-2.44;=0.043)。然而,在两组患者中,与细菌鉴定相关的结局异质性无显著差异,表明合并感染对死亡率的影响在 SARS-CoV-2 患者与流感患者之间无差异。与流感性肺炎患者相比,SARS-CoV-2 肺炎患者在气管插管后 48 小时内进行细菌鉴定的频率显著较低。该临床试验已在 www.clinicaltrials.gov 上注册(NCT04359693)。