The Irish Longitudinal Study on Ageing (TILDA), Trinity College Dublin, Dublin, Ireland.
Department of Population Health Sciences, School of Population Health and Environmental Sciences, King's College London, London, United Kingdom.
PLoS One. 2021 May 27;16(5):e0252212. doi: 10.1371/journal.pone.0252212. eCollection 2021.
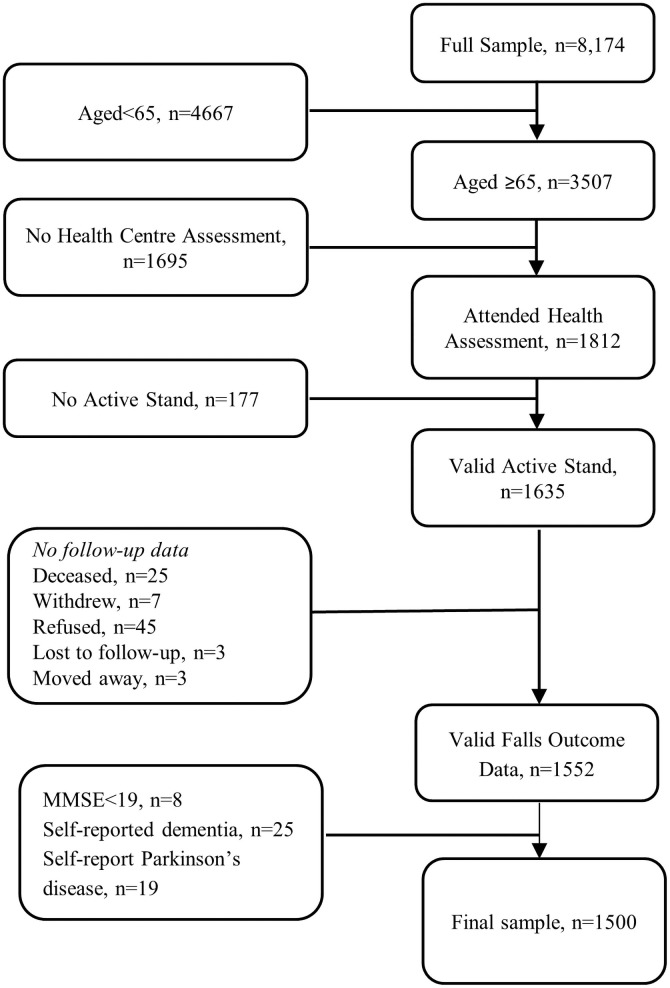
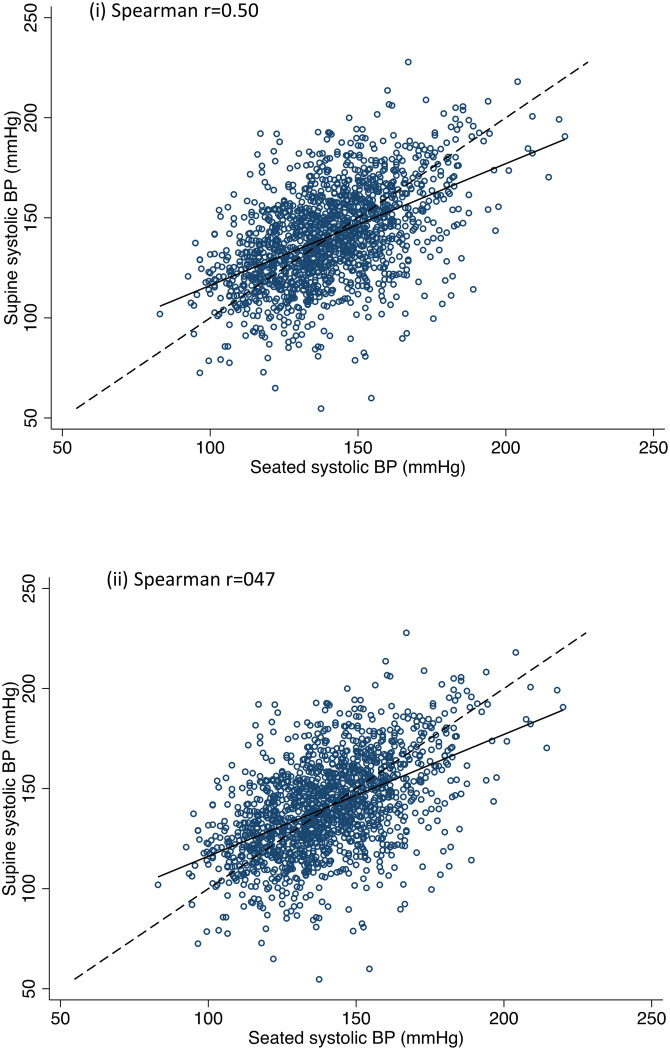
Orthostatic hypotension (OH) often co-exists with hypertension. As increasing age affects baroreflex sensitivity, it loses its ability to reduce blood pressure when lying down. Therefore, supine hypertension may be an important indicator of baroreflex function. This study examines (i) the association between OH and future falls in community-dwelling older adults and (ii) if these associations persist in those with co-existing OH and baseline hypertension, measured supine and seated. Data from 1500 community-dwelling adults aged ≥65 years from The Irish Longitudinal Study on Ageing (TILDA) were used. Continuous beat-to-beat blood pressure was measured using digital photoplethysmography during an active stand procedure with OH defined as a drop in systolic blood pressure (SBP) ≥20 mmHg and/or ≥10 mm Hg in diastolic blood pressure (DBP) within 3 minutes of standing. OH at 40 seconds (OH40) was used as a marker of impaired early stabilisation and OH sustained over the second minute (sustained OH) was used to indicate a more persistent deficit, similar to traditional OH definitions. Seated and supine hypertension were defined as SBP ≥140 mm Hg or DBP ≥90 mm Hg. Modified Poisson models were used to estimate relative risk of falls (recurrent, injurious, unexplained) and syncope occurring over four year follow-up. OH40 was independently associated with recurrent (RR = 1.30, 95% CI = 1.02,1.65), injurious (RR = 1.43, 95% CI = 1.13,1.79) and unexplained falls (RR = 1.55, 95% CI = 1.13,2.13). Sustained OH was associated with injurious (RR = 1.55, 95% CI = 1.18,2.05) and unexplained falls (RR = 1.63, 95% CI = 1.06,2.50). OH and co-existing hypertension was associated with all falls outcomes but effect sizes were consistently larger with seated versus supine hypertension. OH, particularly when co-existing with hypertension, was independently associated with increased risk of future falls. Stronger effect sizes were observed with seated versus supine hypertension. This supports previous findings and highlights the importance of assessing orthostatic blood pressure behaviour in older adults at risk of falls and with hypertension. Observed associations may reflect underlying comorbidities, reduced cerebral perfusion or presence of white matter hyperintensities.
直立性低血压(OH)常与高血压并存。随着年龄的增长,压力反射敏感性下降,当人躺下时,其降低血压的能力丧失。因此,仰卧位高血压可能是压力反射功能的一个重要指标。本研究旨在探讨(i)社区居住的老年人中 OH 与未来跌倒的关系,以及(ii)这些关系是否在同时存在 OH 和基线高血压的患者中仍然存在,这些患者的仰卧位和坐位血压均进行了测量。本研究的数据来自爱尔兰老龄化纵向研究(TILDA)中 1500 名年龄≥65 岁的社区居住成年人。在主动站立过程中,使用数字光体积描记法连续测量每搏血压,OH 的定义为站立 3 分钟内收缩压(SBP)下降≥20mmHg 和/或舒张压(DBP)下降≥10mmHg。使用 OH 40 秒(OH40)作为早期稳定受损的标志物,使用持续站立位 OH(sustained OH)表示更持久的缺陷,类似于传统的 OH 定义。坐位和仰卧位高血压定义为 SBP≥140mmHg 或 DBP≥90mmHg。使用修正泊松模型估计四年随访期间反复、受伤和不明原因跌倒(recurrent,injurious,unexplained)和晕厥的发生风险比(RR)。OH40 与反复(RR=1.30,95%CI=1.02,1.65)、受伤(RR=1.43,95%CI=1.13,1.79)和不明原因跌倒(RR=1.55,95%CI=1.13,2.13)独立相关。持续站立位 OH 与受伤(RR=1.55,95%CI=1.18,2.05)和不明原因跌倒(RR=1.63,95%CI=1.06,2.50)相关。OH 和共存的高血压与所有跌倒结局相关,但坐位高血压的效应大小始终大于仰卧位高血压。OH,特别是与高血压并存时,与未来跌倒风险增加独立相关。与坐位高血压相比,仰卧位高血压观察到的效应更强。这支持了之前的研究结果,并强调了评估有跌倒风险和高血压的老年人直立性血压行为的重要性。观察到的关联可能反映了潜在的共病、脑灌注减少或存在脑白质高信号。