Department of Infection Control and Prevention, The University of Tokyo Hospital, 7-3-1, Hongo, Bunkyo-ku, Tokyo, Japan.
Department of Infectious Diseases, The University of Tokyo Hospital, 7-3-1, Hongo, Bunkyo-ku, Tokyo, Japan.
AIDS Res Ther. 2021 May 27;18(1):30. doi: 10.1186/s12981-021-00354-y.
Antiretrovirals, including tenofovir, can suppress human immunodeficiency virus (HIV) infection but cannot completely eradicate it. Patients with HIV infection are administered antiretroviral drugs over a long term; thus, managing consequent adverse drug reactions, such as renal dysfunction and bone mineral loss, is important. Currently, highly sensitive biomarkers that can detect adverse drug reactions early have not been well studied.
This single-center, prospective, observational study explored changes in the biomarkers of renal function, bone metabolism, and lipid profile before and after switching from tenofovir disoproxil fumarate (TDF) to tenofovir alafenamide (TAF) in patients with HIV infection.
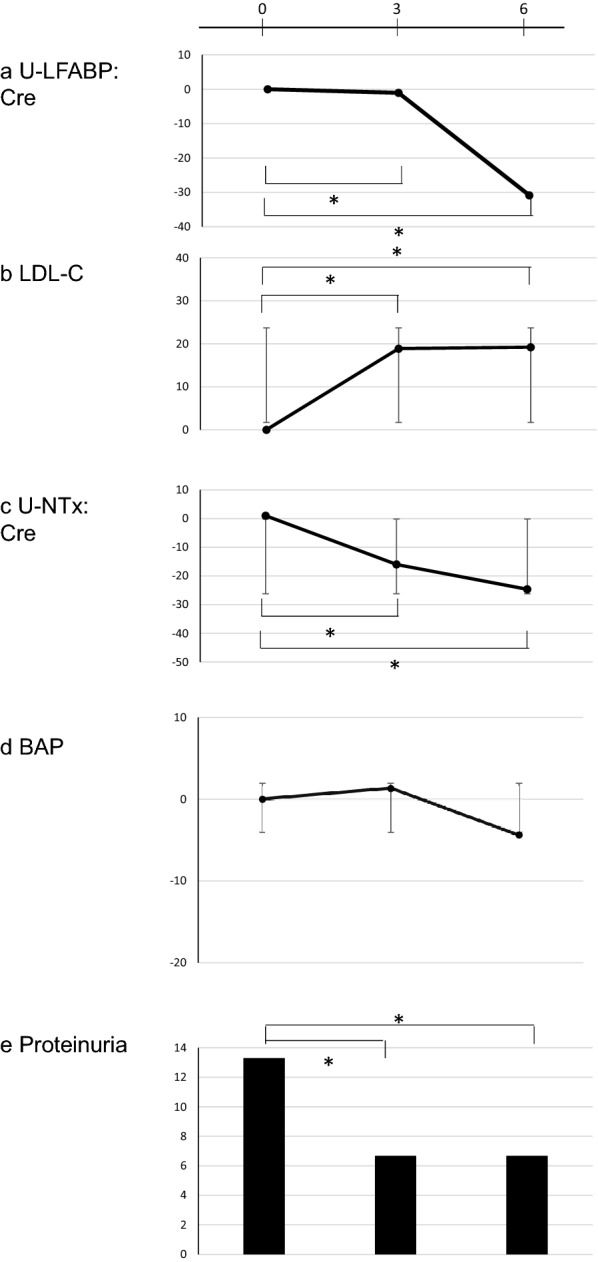
All 31 enrolled patients had been treated with antiretrovirals for more than 5 years. The rate of proteinuria decreased significantly after starting TAF-containing antiretroviral regimen. The urinary liver-type fatty acid binding protein (L-FABP)/creatinine ratio was significantly decreased at 3 and 6 months after switching to TAF compared with that before switching to TAF (- 0.5 μg/g Cr at 3 months, and - 0.8 μg/g Cr at 6 months; p < 005 for both at 3 and 6 months). The urinary N-terminal telopeptide (NTx)/creatinine ratio decreased over the study period, and the ratios were significantly different between 3 and 6 months (- 11 nmol/mmol Cr at 3 months, - 15.2 nmol/mmol Cr at 6 months; p = 0.0069 at 3 months, p < 0.0001 at 6 months). Low density lipoprotein-cholesterol level significantly increased at 3 (+ 26 mg/dL) and 6 months (+ 13 mg/dL) compared with that at the baseline (p < 0.0001).
Switching from TDF to TAF decreased the levels of renal and bone biomarkers, such as urinary L-FABP and NTx, but increased low density lipoprotein-cholesterol levels. Future studies should evaluate if these biomarkers, such as urinary L-FABP and NTx, truly detect serious adverse drug reactions early.
包括替诺福韦在内的抗逆转录病毒药物可以抑制人类免疫缺陷病毒(HIV)感染,但不能将其完全清除。HIV 感染者需要长期服用抗逆转录病毒药物,因此,管理由此产生的不良反应(如肾功能障碍和骨矿物质流失)非常重要。目前,尚未很好地研究出能够早期检测药物不良反应的高灵敏度生物标志物。
本单中心前瞻性观察性研究探讨了 31 例 HIV 感染患者从替诺福韦二吡呋酯(TDF)转换为替诺福韦艾拉酚胺(TAF)后肾功能、骨代谢和血脂谱生物标志物的变化。
所有纳入的 31 例患者均接受抗逆转录病毒治疗超过 5 年。开始含 TAF 的抗逆转录病毒方案后,蛋白尿率显著下降。与转换 TAF 前相比,转换 TAF 后 3 个月和 6 个月时尿肝型脂肪酸结合蛋白(L-FABP)/肌酐比值显著降低(3 个月时降低 0.5μg/gCr,6 个月时降低 0.8μg/gCr;均 p<0.05)。尿 N 末端肽(NTx)/肌酐比值在研究期间下降,3 个月和 6 个月时比值存在显著差异(3 个月时降低 11nmol/mmolCr,6 个月时降低 15.2nmol/mmolCr;均 p=0.0069)。与基线相比,3 个月(+26mg/dL)和 6 个月(+13mg/dL)时低密度脂蛋白胆固醇水平显著升高(均 p<0.0001)。
从 TDF 转换为 TAF 降低了尿 L-FABP 和 NTx 等肾和骨生物标志物的水平,但增加了低密度脂蛋白胆固醇水平。未来的研究应评估这些生物标志物(如尿 L-FABP 和 NTx)是否真的能早期检测到严重的药物不良反应。