Department of Urology, Comprehensive Cancer Center, Vienna General Hospital, Medical University of Vienna, Währinger Gürtel 18-20, 1090, Vienna, Austria.
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia.
World J Urol. 2021 Nov;39(11):4085-4099. doi: 10.1007/s00345-021-03703-8. Epub 2021 May 28.
To summarize the available evidence on the survival and pathologic outcomes after deferred radical prostatectomy (RP) in men with intermediate- and high-risk prostate cancer (PCa).
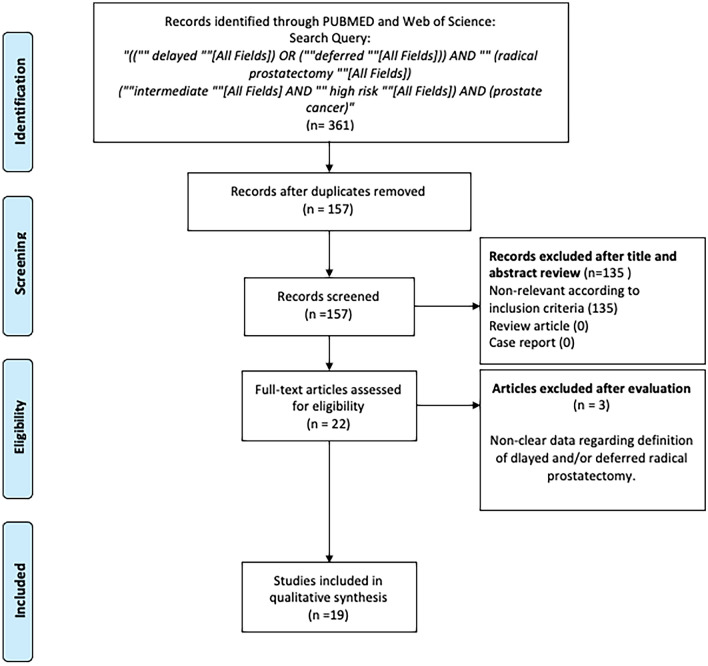
The PubMed database and Web of Science were searched in November 2020 according to the PRISMA statement. Studies were deemed eligible if they reported the survival and pathologic outcomes of patients treated with deferred RP for intermediate- and high-risk PCa compared to the control group including those patients treated with RP without delay.
Overall, nineteen studies met our eligibility criteria. We found a significant heterogeneity across the studies in terms of definitions for delay and outcomes, as well as in patients' baseline clinicopathologic features. According to the currently available literature, deferred RP does not seem to affect oncological survival outcomes, such as prostate cancer-specific mortality and metastasis-free survival, in patients with intermediate- or high-risk PCa. However, the impact of deferred RP on biochemical recurrence rates remains controversial. There is no clear association of deferring RP with any of the features of aggressive disease such as pathologic upgrading, upstaging, positive surgical margins, extracapsular extension, seminal vesicle invasion, and lymph node invasion. Deferred RP was not associated with the need for secondary treatments.
Owing to the different definitions of a delayed RP, it is hard to make a consensus regarding the safe delay time. However, the current data suggest that deferring RP in patients with intermediate- and high-risk PCa for at least around 3 months is generally safe, as it does not lead to adverse pathologic outcomes, biochemical recurrence, the need for secondary therapy, or worse oncological survival outcomes.
总结中高危前列腺癌(PCa)患者延迟根治性前列腺切除术(RP)后的生存和病理结局的现有证据。
根据 PRISMA 声明,于 2020 年 11 月检索 PubMed 数据库和 Web of Science。如果研究报告了与未延迟接受 RP 治疗的对照组相比,接受延迟 RP 治疗的中高危 PCa 患者的生存和病理结局,则认为其符合纳入标准。
共有 19 项研究符合我们的纳入标准。我们发现,在延迟时间和结局的定义以及患者的基线临床病理特征方面,研究之间存在显著的异质性。根据目前的文献,延迟 RP 似乎不会影响中高危 PCa 患者的肿瘤生存结局,如前列腺癌特异性死亡率和无转移生存。然而,延迟 RP 对生化复发率的影响仍存在争议。延迟 RP 与侵袭性疾病的任何特征(如病理升级、分期升级、阳性切缘、包膜外延伸、精囊侵犯和淋巴结侵犯)之间没有明确的关联。延迟 RP 与需要二次治疗无关。
由于延迟 RP 的定义不同,很难就安全的延迟时间达成共识。然而,目前的数据表明,在中高危 PCa 患者中延迟 RP 至少 3 个月通常是安全的,因为它不会导致不良的病理结局、生化复发、需要二次治疗或更差的肿瘤生存结局。