Khasraw Mustafa, Weller Michael, Lorente David, Kolibaba Kathryn, Lee Chee Khoon, Gedye Craig, I de La Fuente Macarena, Vicente David, Reardon David A, Gan Hui K, Scott Andrew M, Dussault Isabelle, Helwig Christoph, Ojalvo Laureen S, Gourmelon Carole, Groves Morris
Royal North Shore Hospital, St Leonards, New South Wales, Australia.
University of Sydney, Sydney, New South Wales, Australia.
Neurooncol Adv. 2021 Apr 9;3(1):vdab058. doi: 10.1093/noajnl/vdab058. eCollection 2021 Jan-Dec.
For patients with recurrent glioblastoma (rGBM), there are few options following treatment failure with radiotherapy plus temozolomide. Bintrafusp alfa is a first-in-class bifunctional fusion protein composed of the extracellular domain of the TGF-βRII receptor (a TGF-β "trap") fused to a human IgG1 antibody blocking PD-L1.
In this phase I, open-label expansion cohort (NCT02517398), patients with rGBM that progressed after radiotherapy plus temozolomide received bintrafusp alfa 1200 mg Q2W until disease progression, unacceptable toxicity, or trial withdrawal. Response was assessed per RANO criteria. The primary endpoint was disease control rate (DCR); secondary endpoints included safety.
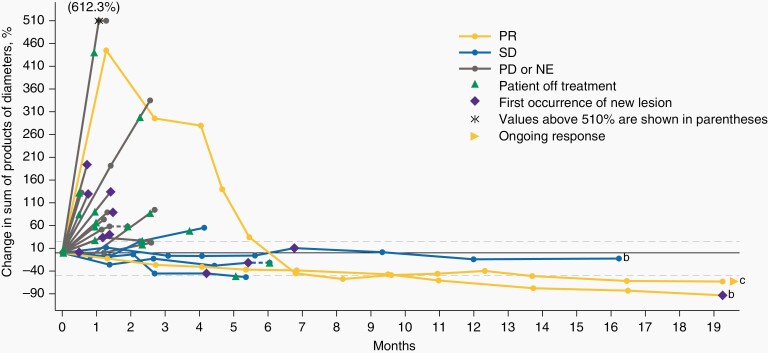
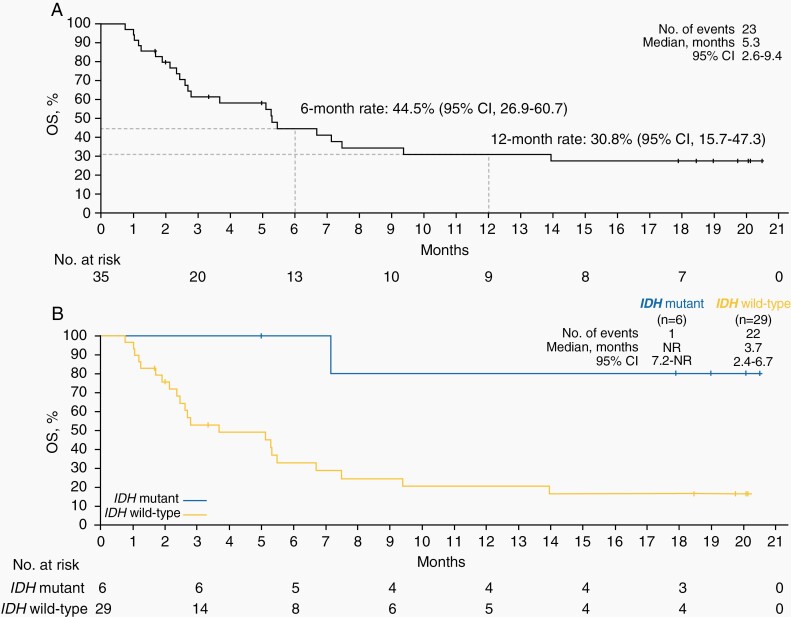
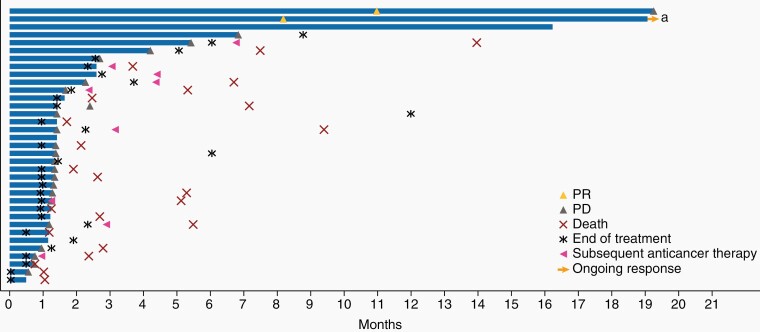
As of August 24, 2018, 35 patients received bintrafusp alfa for a median of 1.8 (range, 0.5-20.7) months. Eight patients (22.9%) experienced disease control as assessed by an independent review committee: 2 had a partial response, 4 had stable disease, and 2 had non-complete response/non-progressive disease. Median progression-free survival (PFS) was 1.4 (95% confidence interval [CI], 1.2-1.6) months; 6- and 12-month PFS rates were 15.1% and 11.3%, respectively. Median overall survival (OS) was 5.3 (95% CI, 2.6-9.4) months; 6- and 12-month OS rates were 44.5% and 30.8%, respectively. The DCR (95% CI) was 66.7% (22.3-95.7%) for patients with -mutant GBM ( = 6) and 13.8% (3.9-31.7%) for patients with -wild-type GBM ( = 29). Disease control was seen regardless of PD-L1 expression. Twenty-five patients (71.4%) experienced treatment-related adverse events (grade ≥3; 17.1% [ = 6]).
The percentage of patients achieving disease control and the manageable safety profile may warrant further investigation of bintrafusp alfa in GBM.
对于复发性胶质母细胞瘤(rGBM)患者,在放疗联合替莫唑胺治疗失败后,治疗选择有限。Bintrafusp alfa是一种一流的双功能融合蛋白,由转化生长因子-βRII受体的细胞外结构域(一种转化生长因子-β“陷阱”)与阻断程序性死亡配体1(PD-L1)的人IgG1抗体融合而成。
在这项I期开放标签扩展队列研究(NCT02517398)中,放疗联合替莫唑胺治疗后病情进展的rGBM患者接受bintrafusp alfa 1200 mg,每2周一次,直至疾病进展、出现不可接受的毒性或试验中止。根据RANO标准评估疗效。主要终点为疾病控制率(DCR);次要终点包括安全性。
截至2018年8月日,35例患者接受了bintrafusp alfa治疗,中位治疗时间为1.8(范围0.5 - 20.7)个月。独立审查委员会评估显示,8例患者(22.9%)病情得到控制:2例部分缓解,4例病情稳定,2例为非完全缓解/疾病未进展。中位无进展生存期(PFS)为1.4(95%置信区间[CI],1.2 - 1.6)个月;6个月和12个月的PFS率分别为15.1%和11.3%。中位总生存期(OS)为5.3(95%CI,2.6 - 9.4)个月;6个月和12个月的OS率分别为44.5%和30.8%。-突变型GBM患者( = 6)的DCR(95%CI)为66.7%(22.3 - 95.7%),-野生型GBM患者( = 29)的DCR为13.8%(3.9 - 31.7%)。无论PD-L1表达情况如何,均观察到病情得到控制。25例患者(71.4%)出现与治疗相关的不良事件(≥3级;17.1%[ = 6])。
实现病情控制的患者比例和可控的安全性可能值得对bintrafusp alfa在GBM中的应用进行进一步研究。