Department of Pulmonary and Critical Care Medicine, Albany Medical Center, 43 New Scotland Avenue, Albany, NY, USA.
Department of Pulmonary and Critical Care, Ozarks Medical Center, West Plains, MO, USA.
Infection. 2021 Dec;49(6):1079-1090. doi: 10.1007/s15010-021-01630-9. Epub 2021 May 31.
Pneumocystis jirovecii (P. jirovecii) is increasingly identified on lower respiratory tract specimens of COVID-19 patients. Our narrative review aims to determine whether the diagnosis of pneumocystis jirovecii pneumonia (PJP) in COVID-19 patients represents coinfection or colonization based on the evidence available in the literature. We also discuss the decision to treat COVID-19 patients with coinfection by PJP.
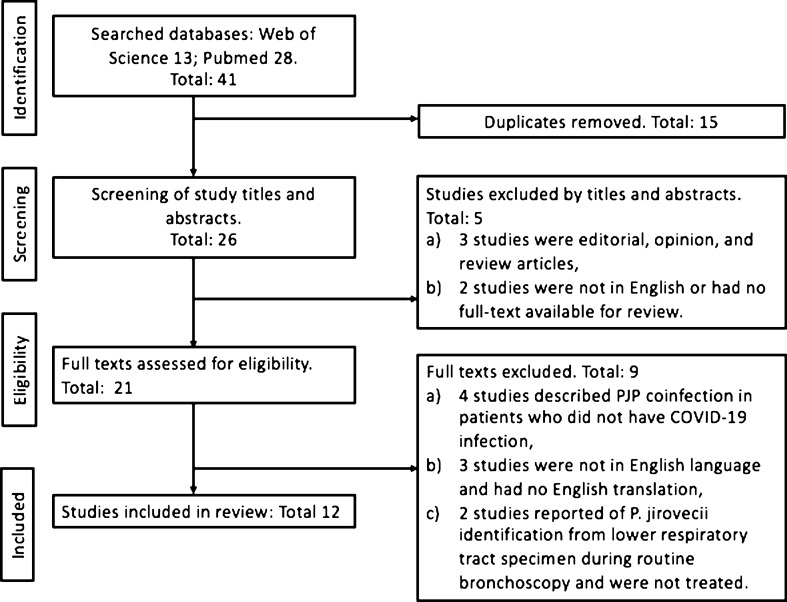
A literature search was performed through the Pubmed and Web of Science databases from inception to March 10, 2021.
We identified 12 COVID-19 patients suspected to have PJP coinfection. All patients were critically ill and required mechanical ventilation. Many were immunosuppressed from HIV or long-term corticosteroids and other immunosuppressive agents. In both the HIV and non-HIV groups, severe lymphocytopenia was encountered with absolute lymphocyte and CD4+T cell count less than 900 and 200 cells/mm, respectively. The time to PJP diagnosis from the initial presentation was 7.8 (range 2-21) days. Serum lactate dehydrogenase and beta-D-glucan were elevated in those coinfected with PJP. All patients were treated with anti-PJP therapy, predominantly sulfamethoxazole-trimethoprim with corticosteroids. The overall mortality rate was 41.6%, and comparable for both HIV and non-HIV groups.
As the current evidence is restricted to case reports, the true incidence, risk factors, and prognosis of COVID-19 patients with PJP coinfections cannot be accurately determined. Comorbidities of poorly controlled HIV with lymphocytopenia and multiple immunosuppressive therapies are likely predisposing factors for PJP coinfection.
肺孢子菌(Pneumocystis jirovecii,P. jirovecii)在 COVID-19 患者的下呼吸道标本中越来越多地被检出。本叙述性综述旨在根据现有文献中的证据,确定 COVID-19 患者肺孢子菌肺炎(PJP)的诊断是合并感染还是定植。我们还讨论了治疗 COVID-19 合并 PJP 感染患者的决策。
通过 Pubmed 和 Web of Science 数据库进行文献检索,检索时间从建库至 2021 年 3 月 10 日。
我们共发现 12 例疑似 COVID-19 患者合并 PJP 感染。所有患者均为重症,需要机械通气。许多患者因 HIV 或长期使用皮质类固醇和其他免疫抑制剂而免疫抑制。在 HIV 组和非 HIV 组中,均出现严重的淋巴细胞减少症,绝对值淋巴细胞和 CD4+T 细胞计数分别小于 900 和 200 个细胞/mm。从最初表现到 PJP 诊断的时间为 7.8(范围 2-21)天。合并 PJP 感染的患者血清乳酸脱氢酶和 β-D-葡聚糖升高。所有患者均接受抗 PJP 治疗,主要是磺胺甲噁唑-甲氧苄啶联合皮质类固醇。总死亡率为 41.6%,在 HIV 组和非 HIV 组中相似。
由于目前的证据仅限于病例报告,因此无法准确确定 COVID-19 合并 PJP 感染患者的真实发病率、危险因素和预后。未经控制的 HIV 合并淋巴细胞减少症和多种免疫抑制剂治疗的合并症可能是 PJP 合并感染的易感因素。