Stege Henner, Haist Maximilian, Schultheis Michael, Fleischer Maria Isabel, Mohr Peter, Meier Friedegund, Schadendorf Dirk, Ugurel Selma, Livingstone Elisabeth, Zimmer Lisa, Herbst Rudolf, Pföhler Claudia, Kähler Katharina, Weichenthal Michael, Terheyden Patrick, Nashan Dorothée, Debus Dirk, Kaatz Martin, Ziller Fabian, Haferkamp Sebastian, Forschner Andrea, Leiter Ulrike, Kreuter Alexander, Ulrich Jens, Kleemann Johannes, Bradfisch Fabienne, Grabbe Stephan, Loquai Carmen
Department of Dermatology, University Medical Center Mainz, 55131 Mainz, Germany.
Department of Dermatology, Elbe Kliniken Buxtehude, 21614 Buxtehude, Germany.
Cancers (Basel). 2021 May 12;13(10):2312. doi: 10.3390/cancers13102312.
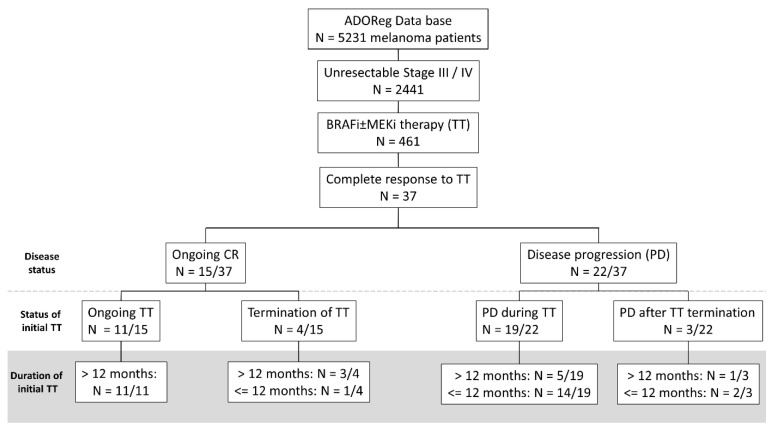
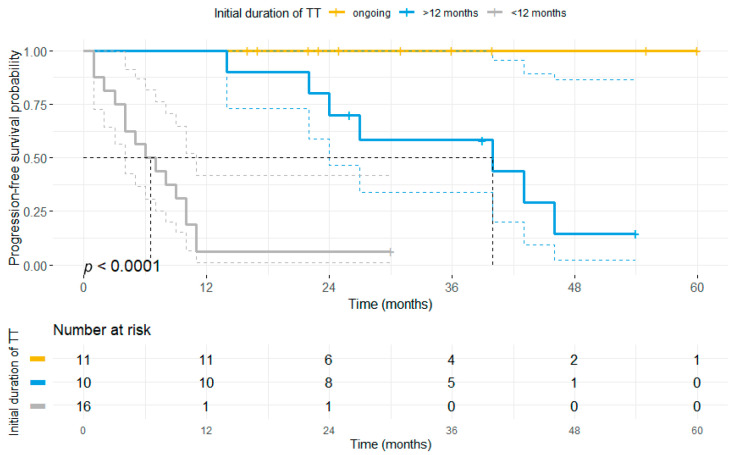
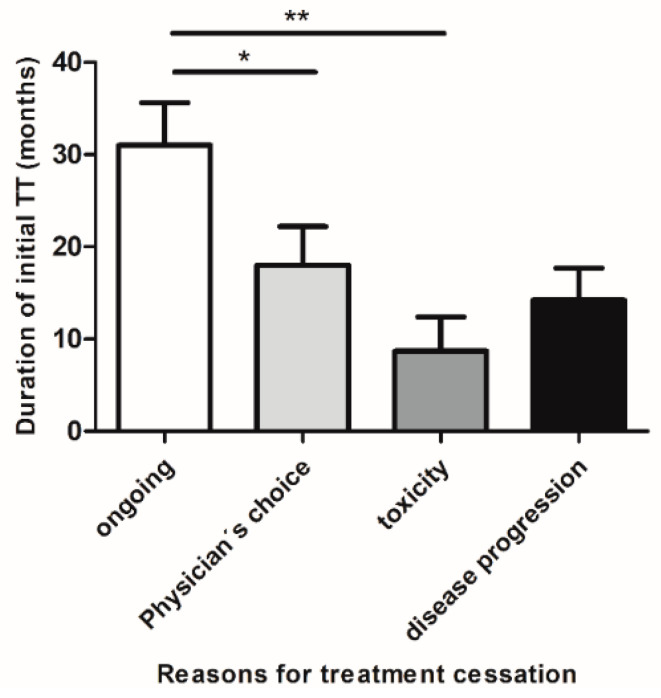
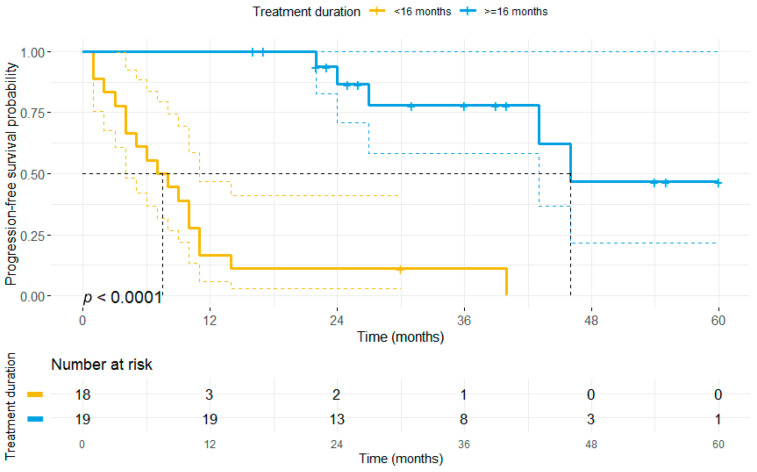
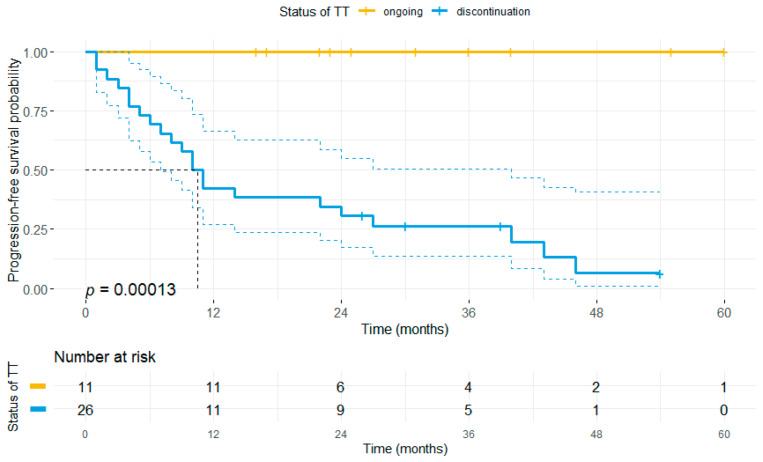
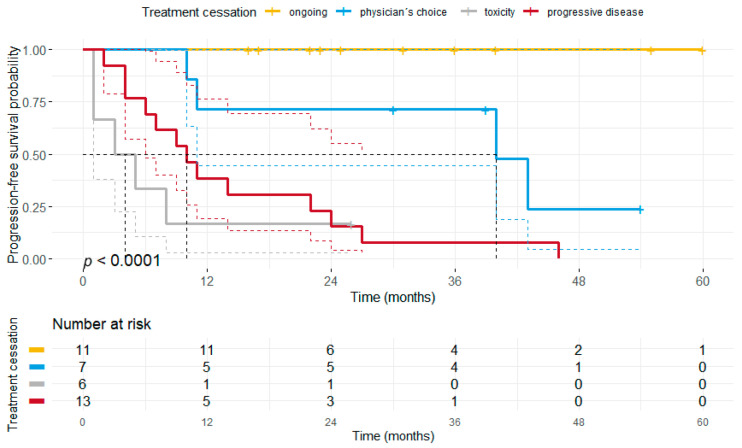
The advent of BRAF/MEK inhibitors (BRAFi/MEKi) has significantly improved progression-free (PFS) and overall survival (OS) for patients with advanced BRAF-V600-mutant melanoma. Long-term survivors have been identified particularly among patients with a complete response (CR) to BRAF/MEK-directed targeted therapy (TT). However, it remains unclear which patients who achieved a CR maintain a durable response and whether treatment cessation might be a safe option in these patients. Therefore, this study investigated the impact of treatment cessation on the clinical course of patients with a CR upon BRAF/MEK-directed-TT. We retrospectively selected patients with BRAF-V600-mutant advanced non-resectable melanoma who had been treated with BRAFi ± MEKi therapy and achieved a CR upon treatment out of the multicentric skin cancer registry ADOReg. Data on baseline patient characteristics, duration of TT, treatment cessation, tumor progression (TP) and response to second-line treatments were collected and analyzed. Of 461 patients who received BRAF/MEK-directed TT 37 achieved a CR. TP after initial CR was observed in 22 patients (60%) mainly affecting patients who discontinued TT (n = 22/26), whereas all patients with ongoing TT (n = 11) maintained their CR. Accordingly, patients who discontinued TT had a higher risk of TP compared to patients with ongoing treatment ( < 0.001). However, our data also show that patients who received TT for more than 16 months and who discontinued TT for other reasons than TP or toxicity did not have a shorter PFS compared to patients with ongoing treatment. Response rates to second-line treatment being initiated in 21 patients, varied between 27% for immune-checkpoint inhibitors (ICI) and 60% for BRAFi/MEKi rechallenge. In summary, we identified a considerable number of patients who achieved a CR upon BRAF/MEK-directed TT in this contemporary real-world cohort of patients with BRAF-V600-mutant melanoma. Sustained PFS was not restricted to ongoing TT but was also found in patients who discontinued TT.
BRAF/MEK抑制剂(BRAFi/MEKi)的出现显著改善了晚期BRAF-V600突变黑色素瘤患者的无进展生存期(PFS)和总生存期(OS)。长期生存者尤其在对BRAF/MEK靶向治疗(TT)有完全缓解(CR)的患者中被发现。然而,尚不清楚哪些达到CR的患者能维持持久缓解,以及在这些患者中停止治疗是否可能是一个安全的选择。因此,本研究调查了停止治疗对接受BRAF/MEK靶向TT且达到CR的患者临床病程的影响。我们从多中心皮肤癌登记处ADOReg中回顾性选择了接受BRAFi±MEKi治疗且在治疗后达到CR的BRAF-V600突变晚期不可切除黑色素瘤患者。收集并分析了患者基线特征、TT持续时间、停止治疗、肿瘤进展(TP)及二线治疗反应的数据。在461例接受BRAF/MEK靶向TT的患者中,37例达到CR。22例(60%)患者在初始CR后出现TP,主要影响停止TT的患者(22/26),而所有继续接受TT的患者(11例)维持CR。因此,与继续治疗的患者相比,停止TT的患者TP风险更高(<0.001)。然而,我们的数据还显示,接受TT超过16个月且因TP或毒性以外的其他原因停止TT的患者与继续治疗的患者相比,PFS并无缩短。21例患者开始二线治疗的反应率各不相同,免疫检查点抑制剂(ICI)为27%,BRAFi/MEKi再挑战为60%。总之,在这个当代BRAF-V600突变黑色素瘤患者的真实世界队列中,我们发现相当数量的患者在接受BRAF/MEK靶向TT后达到CR。持续的PFS不仅限于继续接受TT的患者,在停止TT的患者中也有发现。