ICES, Toronto, Ontario, Canada.
Department of Physical Therapy, University of Toronto, Toronto, Ontario, Canada.
BMJ Open. 2021 Jun 1;11(6):e042978. doi: 10.1136/bmjopen-2020-042978.
To compare recent immigrants and long-term residents in Ontario, Canada, on established health service quality indicators of end-of-life cancer care.
Retrospective, population-based cohort study of cancer decedents between 2004 and 2015.
Ontario, Canada.
We grouped 13 085 immigrants who arrived in Ontario in 1985 or later into eight major ethnic groups based on birth country, mother tongue and surname, and compared them to 229 471 long-term residents who were ≥18 years at the time of death.
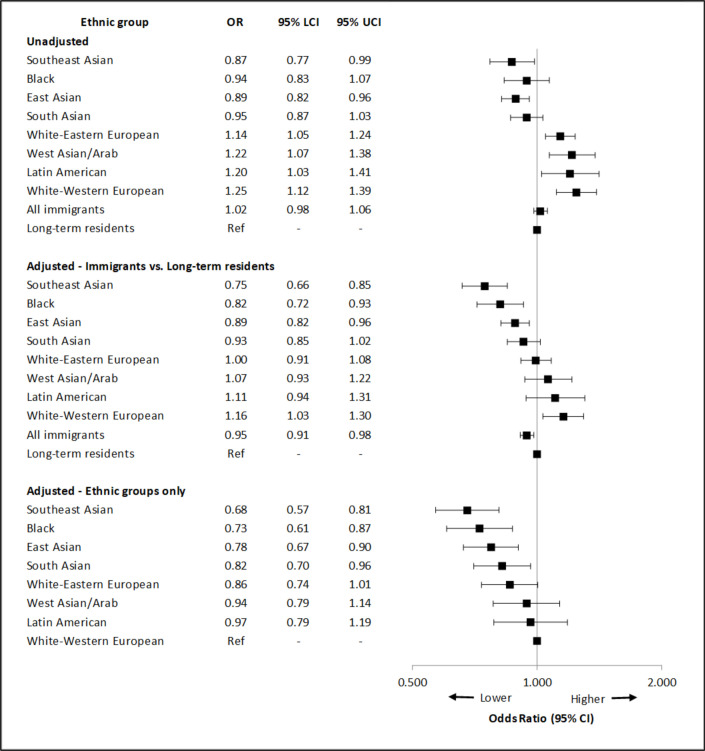
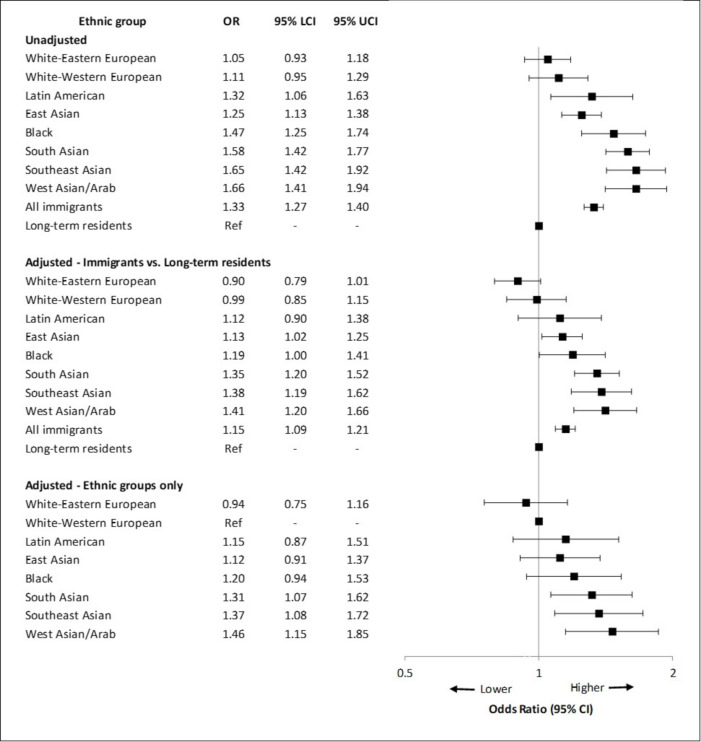
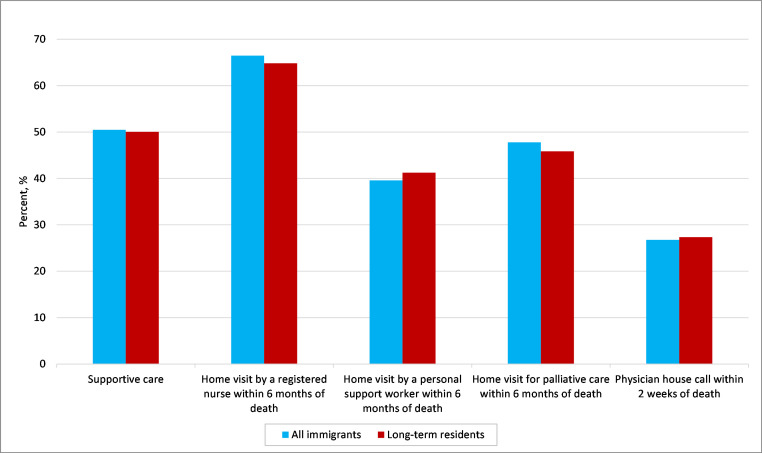
Aggressive care, defined as a composite of ≥2 emergency department visits, ≥2 new hospitalisations or an intensive care unit admission within 30 days of death; and supportive care, defined as a physician house call within 2 weeks, or palliative nursing or personal support worker home visit within 6 months of death. Multivariable logistic regression was used to examine the association between immigration status and the odds of each main outcome.
Compared with long-term residents, immigrants overall and by ethnic group had higher rates of aggressive care (13.7% vs 17.5%, respectively; p<0.001). Among immigrants, Southeast Asians had the highest use while White-Eastern and Western Europeans had the lowest. Supportive care use was similar between long-term residents and immigrants (50.0% vs 50.5%, respectively; p=0.36), though lower among Southeast Asians (46.6%) and higher among White-Western Europeans (55.6%). After adjusting for sociodemographic characteristics and comorbidities, immigrants remained more likely than long-term residents to receive aggressive care (OR: 1.15, 95% CI 1.09 to 1.21), yet were less likely to receive supportive care (OR: 0.95, 95% CI 0.91 to 0.98).
Among cancer decedents in Ontario, immigrants are more likely to use aggressive healthcare services at the end of life than long-term residents, while supportive care varies by ethnicity. Contributors to variation in end-of-life care require further study.
比较加拿大安大略省的近期移民和长期居民在癌症临终关怀既定健康服务质量指标方面的情况。
2004 年至 2015 年间基于癌症死亡患者的回顾性、基于人群的队列研究。
加拿大安大略省。
我们根据出生国、母语和姓氏将 13085 名于 1985 年或之前抵达安大略省的移民分为八个主要族裔群体,并将他们与 229471 名死亡时年龄在 18 岁及以上的长期居民进行比较。
侵袭性护理,定义为死亡后 30 天内≥2 次急诊就诊、≥2 次新住院或入住重症监护病房;支持性护理,定义为医生上门就诊、2 周内姑息护理或个人支持工作者上门就诊,死亡后 6 个月内。多变量逻辑回归用于检查移民身份与每种主要结局的几率之间的关联。
与长期居民相比,总体而言,移民和按族裔群体的侵袭性护理使用率更高(分别为 13.7%和 17.5%;均<0.001)。在移民中,东南亚裔的使用率最高,而白种-东欧和西欧裔的使用率最低。长期居民和移民的支持性护理使用率相似(分别为 50.0%和 50.5%;p=0.36),尽管东南亚裔的使用率较低(46.6%),而白种-西欧裔的使用率较高(55.6%)。在调整社会人口统计学特征和合并症后,移民接受侵袭性护理的可能性仍高于长期居民(比值比:1.15,95%置信区间:1.09 至 1.21),但接受支持性护理的可能性较低(比值比:0.95,95%置信区间:0.91 至 0.98)。
在安大略省的癌症死亡患者中,与长期居民相比,移民在生命末期更有可能使用侵袭性医疗服务,而支持性护理则因族裔而异。需要进一步研究导致临终关怀差异的因素。