Chen Jia, Ni Hai-Jian, Xue Fei, Fan Yun-Shan, Li Xi-Fan, Chen Xian-Zhen, He Shi-Sheng
Department of Orthopaedics, Shanghai Tenth People's Hospital, Tongji University School of Medicine, Shanghai, 200072, People's Republic of China.
Spinal Pain Research Institute, Tongji University School of Medicine, Shanghai, 200072, People's Republic of China.
J Pain Res. 2021 May 27;14:1475-1481. doi: 10.2147/JPR.S297304. eCollection 2021.
Intradural disc herniation (IDH) is a rare type of disc degeneration that infrequently affects the upper lumbar spine. Pre- and intraoperative diagnosis and surgical management of IDH are challenging. The present case study provides insight into these aspects of upper lumbar IDH and discusses possible mechanisms.
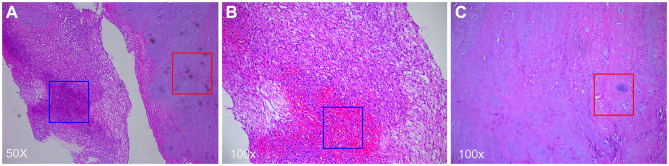
A 63-year-old female with a history of chronic lower back and leg pain presented with an acute lumbar sprain that had occurred 1 month prior. The pain progressed and spread to the front of the left thigh, which affected her ability to lift her leg when ascending/descending stairs. Sagittal gadolinium-enhanced magnetic resonance imaging (MRI) revealed a disc protruding into the ventral dural sac showing a hawk-beak sign, and the posterior edge of the disc annulus and local posterior longitudinal ligament was broken. Total L2 laminectomy was performed, and the dorsal side of the dural sac was exposed and incised to enable exploration of the ventral side of the dura. We found two free fragments protruding into the inner wall of the dura through the left ventral dura mater defect. After carefully and completely removing the mass, we repaired the defect and performed internal fixation. Postoperative pathologic analysis confirmed that the mass was nucleus pulposus tissue from the degenerated disc. The patient's pain significantly improved after surgery, and she was able to walk normally at the 1-month follow-up.
Upper lumbar IDH is an extremely rare type of disc degeneration. An enhanced MRI scan can provide diagnostic evidence, but the final diagnosis requires surgical exploration of the path of herniation and pathologic examination of the mass lesion.
硬脊膜内椎间盘突出症(IDH)是一种罕见的椎间盘退变类型,很少影响上腰椎。IDH的术前和术中诊断及手术治疗具有挑战性。本病例研究深入探讨了上腰椎IDH的这些方面,并讨论了可能的机制。
一名63岁女性,有慢性腰腿痛病史,1个月前出现急性腰扭伤。疼痛加重并蔓延至左大腿前部,影响她上下楼梯时抬腿的能力。矢状位钆增强磁共振成像(MRI)显示一个椎间盘突入腹侧硬脊膜囊,呈鹰喙征,椎间盘环的后缘和局部后纵韧带断裂。行L2全椎板切除术,暴露并切开硬脊膜囊的背侧,以便探查硬脊膜的腹侧。我们发现两个游离碎片通过左腹侧硬脊膜缺损突入硬脊膜内壁。仔细彻底切除肿块后,我们修复了缺损并进行了内固定。术后病理分析证实肿块为退变椎间盘的髓核组织。患者术后疼痛明显改善,1个月随访时能够正常行走。
上腰椎IDH是一种极其罕见的椎间盘退变类型。增强MRI扫描可提供诊断依据,但最终诊断需要对突出路径进行手术探查及对肿块病变进行病理检查。