Said Samar M, Rocha Alejandro Best, Valeri Anthony M, Sandid Mohamad, Ray Anhisekh Sinha, Fidler Mary E, Alexander Mariam Priya, Larsen Christopher P, Nasr Samih H
Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, USA.
Arkana Laboratories, Little Rock, AR, USA.
Clin Kidney J. 2020 Dec 5;14(6):1681-1690. doi: 10.1093/ckj/sfaa205. eCollection 2021 Jun.
Coexistence of fibrillary glomerulonephritis (FGN) and immunoglobulin A (IgA) nephropathy (IgAN) in the same kidney biopsy (FGN-IgAN) is rare, and the clinicopathologic characteristics and outcome of this dual glomerulopathy are unknown.
In this study, 20 patients with FGN-IgAN were studied and their characteristics were compared with 40 FGN and 40 IgAN control patients.
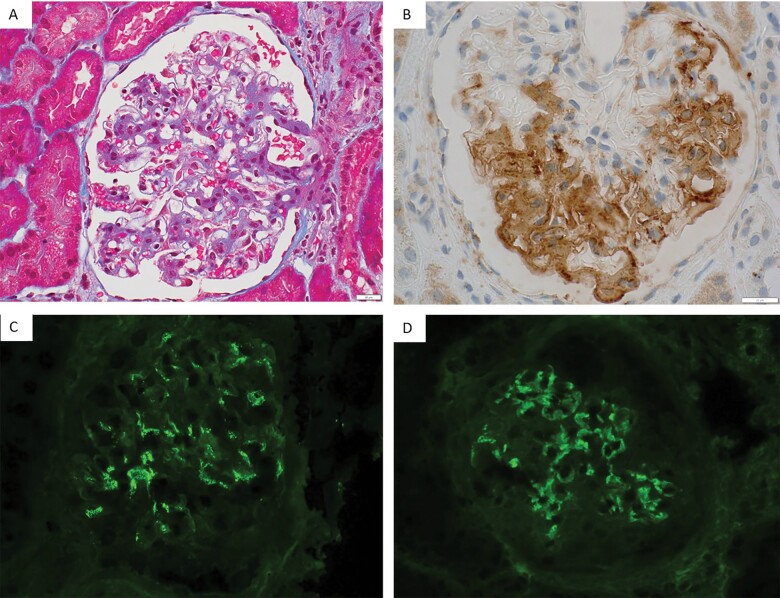
Concurrent IgAN was present in 1.8% of 847 consecutive FGN cases and was the second most common concurrent glomerulopathy after diabetic nephropathy. FGN-IgAN patients were overwhelmingly White (94%) and contrary to FGN patients were predominantly (60%) males. Compared with IgAN patients, FGN-IgAN patients were older, had higher proteinuria, a higher incidence of renal insufficiency, and a lower incidence of microhematuria and gross hematuria at diagnosis. Six (30%) patients had malignancy, autoimmune disease or hepatitis C infection, but none had a secondary cause of IgAN or clinical features of Henoch-Schonlein purpura. Histologically, all cases exhibited smudgy glomerular staining for immunoglobulin G and DnaJ homolog subfamily B member 9 (DNAJB9) with corresponding fibrillary deposits and granular mesangial staining for IgA with corresponding mesangial granular electron-dense deposits. On follow-up (median 27 months), 10 of 18 (56%) FGN-IgAN patients progressed to end-stage kidney disease (ESKD), including 5 who subsequently died. Serum creatinine at diagnosis was a poor predictor of renal survival. The proportion of patients reaching ESKD or died was higher in FGN-IgAN than in IgAN. The median Kaplan-Meier ESKD-free survival time was 44 months for FGN-IgAN, which was shorter than IgAN (unable to compute, P =0.013) and FGN (107 months, P = 0.048).
FGN-IgAN is very rare, with clinical presentation and demographics closer to FGN than IgAN. Prognosis is guarded with a median renal survival of 3.6 years. The diagnosis of this dual glomerulopathy requires careful evaluation of immunofluorescence findings, and electron microscopy or DNAJB9 immunohistochemistry.
在同一肾脏活检标本中,纤维性肾小球肾炎(FGN)与免疫球蛋白A(IgA)肾病(IgAN)并存(FGN-IgAN)的情况较为罕见,这种双重肾小球病的临床病理特征及预后尚不清楚。
本研究纳入了20例FGN-IgAN患者,并将其特征与40例FGN患者及40例IgAN对照患者进行比较。
在847例连续的FGN病例中,IgAN并发率为1.8%,是继糖尿病肾病之后第二常见的并发肾小球病。FGN-IgAN患者绝大多数为白人(94%),与FGN患者相反,主要为男性(60%)。与IgAN患者相比,FGN-IgAN患者年龄更大,蛋白尿更多,肾功能不全发生率更高,诊断时镜下血尿和肉眼血尿发生率更低。6例(30%)患者患有恶性肿瘤、自身免疫性疾病或丙型肝炎感染,但均无IgAN的继发原因或过敏性紫癜的临床特征。组织学上,所有病例均表现为肾小球免疫球蛋白G和DnaJ同源亚家族B成员9(DNAJB9)呈模糊染色,伴有相应的纤维样沉积物,IgA呈颗粒状系膜染色,伴有相应的系膜颗粒状电子致密沉积物。随访(中位时间27个月)时,18例FGN-IgAN患者中有10例(56%)进展至终末期肾病(ESKD),其中5例随后死亡。诊断时的血清肌酐对肾脏生存的预测价值较差。FGN-IgAN患者进展至ESKD或死亡的比例高于IgAN患者。FGN-IgAN患者的中位Kaplan-Meier无ESKD生存时间为44个月,短于IgAN患者(无法计算,P = 0.013)和FGN患者(107个月,P = 0.048)。
FGN-IgAN非常罕见,其临床表现和人口统计学特征更接近FGN而非IgAN。预后不佳,中位肾脏生存时间为3.6年。这种双重肾小球病的诊断需要仔细评估免疫荧光结果,并结合电子显微镜检查或DNAJB9免疫组织化学检查。