Yu Han, Del Nido Pedro J, Geva Tal, Yang Chun, Wu Zheyang, Rathod Rahul H, Huang Xueying, Billiar Kristen L, Tang Dalin
School of Biological Science and Medical Engineering, Southeast University, Nanjing, China.
Department of Cardiac Surgery, Boston Children's Hospital, Boston, MA, United States.
Front Bioeng Biotechnol. 2021 May 19;9:638934. doi: 10.3389/fbioe.2021.638934. eCollection 2021.
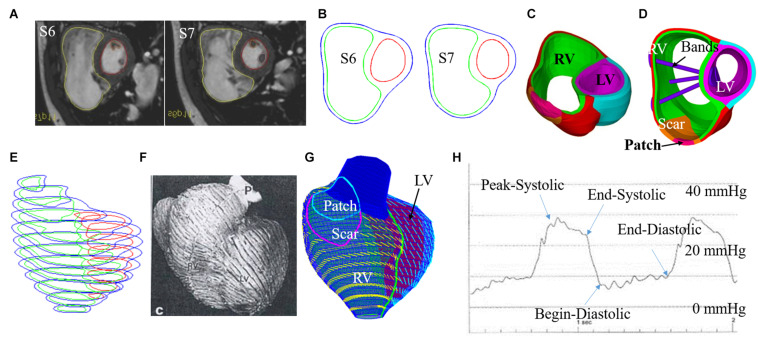
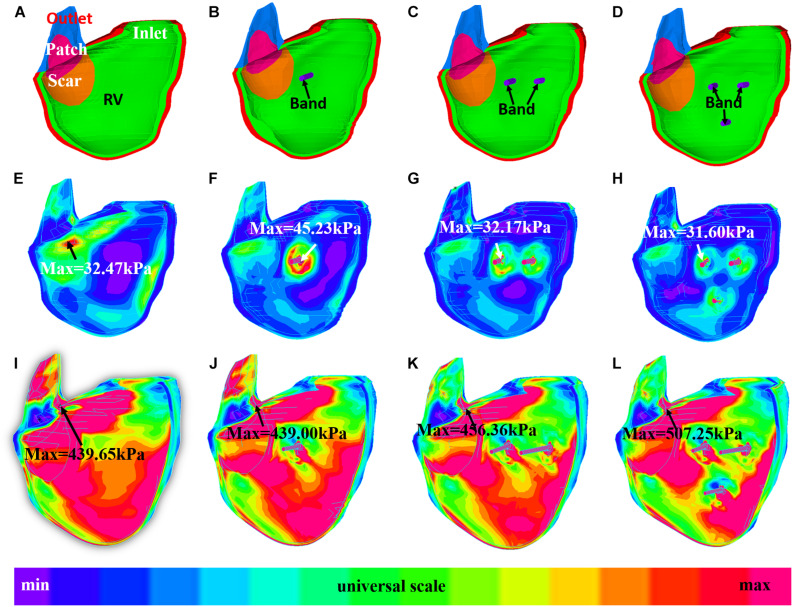
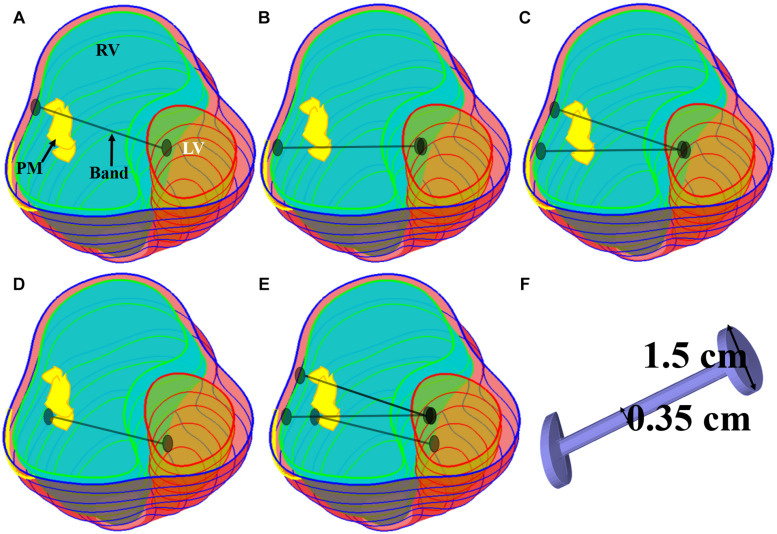
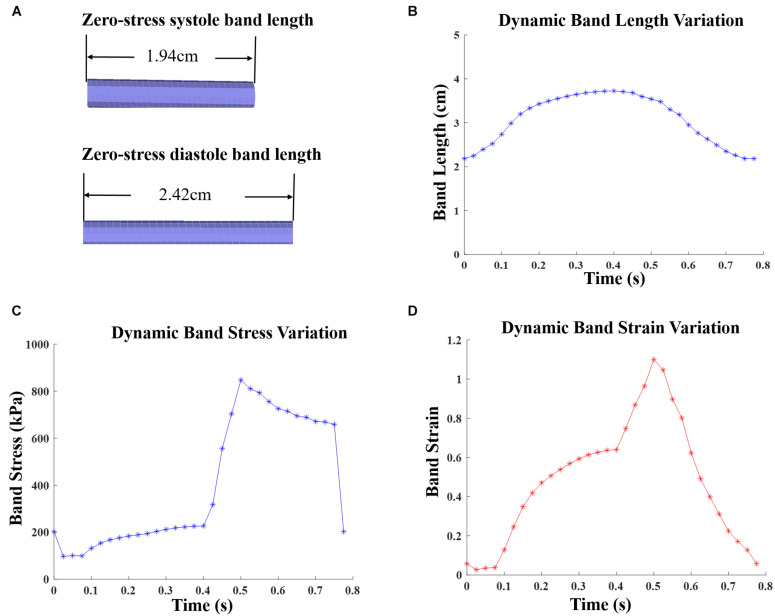
Patients with repaired Tetralogy of Fallot (ToF), a congenital heart defect which includes a ventricular septal defect and severe right ventricular outflow obstruction, account for the majority of cases with late-onset right ventricle (RV) failure. Current surgery procedures, including pulmonary valve replacement (PVR) with right ventricle remodeling, yield mixed results. PVR with active band insertion was hypothesized to be of clinical usage on improving RV function measured by ejection fraction (EF). In lieu of risky open-heart surgeries and experiments on animal and human, computational biomechanical models were adapted to study the impact of PVR with five band insertion options. Cardiac magnetic resonance (CMR) images were acquired from seven TOF patients before PVR surgery for model construction. For each patient, five different surgery plans combined with passive and active contraction band with contraction ratio of 20, 15, and 10% were studied. Those five plans include three single-band plans with different band locations; one plan with two bands, and one plan with three bands. Including the seven no-band models, 147 computational bi-ventricle models were constructed to simulate RV cardiac functions and identify optimal band plans. Patient variations with different band plans were investigated. Surgery plan with three active contraction bands and band active contraction ratio of 20% had the best performance on improving RV function. The mean ± SD RV ejection fraction value from the seven patients was 42.90 ± 5.68%, presenting a 4.19% absolute improvement or a 10.82% relative improvement, when compared with the baseline models (38.71 ± 5.73%, = 0.016). The EF improvements from the seven patients varied from 2.87 to 6.01%. Surgical procedures using active contraction bands have great potential to improve RV function measured by ejection fraction for patients with repaired ToF. It is possible to have higher right ventricle ejection fraction improvement with more bands and higher band active contraction ratio. Our findings with computational models need to be further validated by animal experiments before clinical trial could become possible.
法洛四联症(ToF)修复患者中,法洛四联症是一种先天性心脏缺陷,包括室间隔缺损和严重的右心室流出道梗阻,占晚期右心室(RV)衰竭病例的大多数。目前的手术程序,包括右心室重塑的肺动脉瓣置换术(PVR),效果不一。有人假设,插入主动带的PVR在改善以射血分数(EF)衡量的右心室功能方面具有临床应用价值。为了避免危险的心脏直视手术以及在动物和人体上进行实验,采用了计算生物力学模型来研究五种带插入选项的PVR的影响。在PVR手术前,从7名ToF患者获取心脏磁共振(CMR)图像用于模型构建。对于每位患者,研究了五种不同的手术方案,这些方案结合了收缩率为20%、15%和10%的被动和主动收缩带。这五种方案包括三个不同带位置的单带方案;一个双带方案和一个三带方案。包括七个无带模型,共构建了147个计算双心室模型来模拟右心室心脏功能并确定最佳带方案。研究了不同带方案下的患者差异。具有三个主动收缩带且带主动收缩率为20%的手术方案在改善右心室功能方面表现最佳。与基线模型(38.71±5.73%,P = 0.016)相比,这7名患者的平均±标准差右心室射血分数值为42.90±5.68%,绝对改善4.19%,相对改善10.82%。这7名患者的EF改善幅度从2.87%到6.01%不等。对于法洛四联症修复患者,使用主动收缩带的手术程序在改善以射血分数衡量的右心室功能方面具有很大潜力。使用更多的带和更高的带主动收缩率可能会使右心室射血分数有更高的改善。在进行临床试验之前,我们通过计算模型得出的结果需要通过动物实验进一步验证。