Division of Cardiac Critical Care Department of Pediatrics Medical City Children's Hospital Dallas TX.
ZOLL Medical Corporation Chelmsford MA.
J Am Heart Assoc. 2021 Jun 15;10(12):e020353. doi: 10.1161/JAHA.120.020353. Epub 2021 Jun 5.
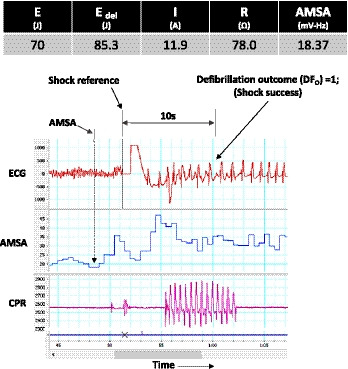
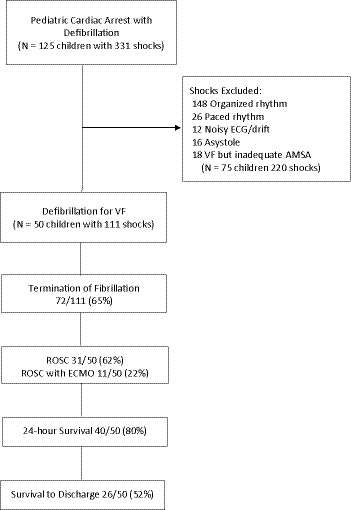
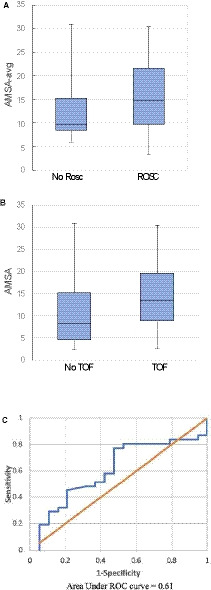
Background Amplitude spectral area (AMSA) predicts termination of fibrillation (TOF) with return of spontaneous circulation (ROSC) and survival in adults but has not been studied in pediatric cardiac arrest. We characterized AMSA during pediatric cardiac arrest from a Pediatric Resuscitation Quality Collaborative and hypothesized that AMSA would be associated with TOF and ROSC. Methods and Results Children aged <18 years with cardiac arrest and ventricular fibrillation were studied. AMSA was calculated for 2 seconds before shock and averaged for each subject (AMSA-avg). TOF was defined as termination of ventricular fibrillation 10 seconds after defibrillation to any non-ventricular fibrillation rhythm. ROSC was defined as >20 minutes without chest compressions. Univariate and multivariable logistic regression analyses controlling for weight, current, and illness category were performed. Primary end points were TOF and ROSC. Secondary end points were 24-hour survival and survival to discharge. Between 2015 and 2019, 50 children from 14 hospitals with 111 shocks were identified. In univariate analyses AMSA was not associated with TOF and AMS-Aavg was not associated with ROSC. Multivariable logistic regression showed no association between AMSA and TOF but controlling for defibrillation average current and illness category, there was a trend to significant association between AMSA-avg and ROSC (odds ratio, 1.10 [1.00‒1.22] =0.058). There was no significant association between AMSA-avg and 24-hour survival or survival to hospital discharge. Conclusions In pediatric patients, AMSA was not associated with TOF, whereas AMSA-avg had a trend to significance for association in ROSC, but not 24-hour survival or survival to hospital discharge. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02708134.
背景
振幅谱面积 (AMSA) 可预测成人纤颤终止 (TOF) 和自主循环恢复 (ROSC),但尚未在儿科心搏骤停中进行研究。我们从儿科复苏质量协作组织中描述了儿科心搏骤停期间的 AMSA,并假设 AMSA 与 TOF 和 ROSC 相关。
方法和结果
研究了年龄<18 岁的有心搏骤停和室颤的儿童。在电击前计算 2 秒的 AMSA 并对每个患者进行平均(AMSA-avg)。TOF 定义为除室颤外的任何非室颤节律电击后 10 秒终止。ROSC 定义为>20 分钟无胸外按压。进行了单变量和多变量逻辑回归分析,控制体重、电流和疾病类别。主要终点是 TOF 和 ROSC。次要终点是 24 小时生存率和出院生存率。在 2015 年至 2019 年期间,从 14 家医院的 111 次电击中确定了 50 名儿童。在单变量分析中,AMSA 与 TOF 无关,AMSA-avg 与 ROSC 无关。多变量逻辑回归显示,AMSA 与 TOF 之间无关联,但控制除颤平均电流和疾病类别后,AMSA-avg 与 ROSC 之间存在显著关联的趋势(比值比,1.10[1.00-1.22]=0.058)。AMSA-avg 与 24 小时生存率或出院生存率之间无显著关联。
结论
在儿科患者中,AMSA 与 TOF 无关,而 AMSA-avg 与 ROSC 相关有显著趋势,但与 24 小时生存率或出院生存率无关。