Department of Cardiology Bern University Hospital Bern Switzerland.
Division of Cardiology Department of Translational Medicine University of Campania "Luigi Vanvitelli Caserta Italy.
J Am Heart Assoc. 2021 Jun 15;10(12):e021965. doi: 10.1161/JAHA.121.021965. Epub 2021 Jun 8.
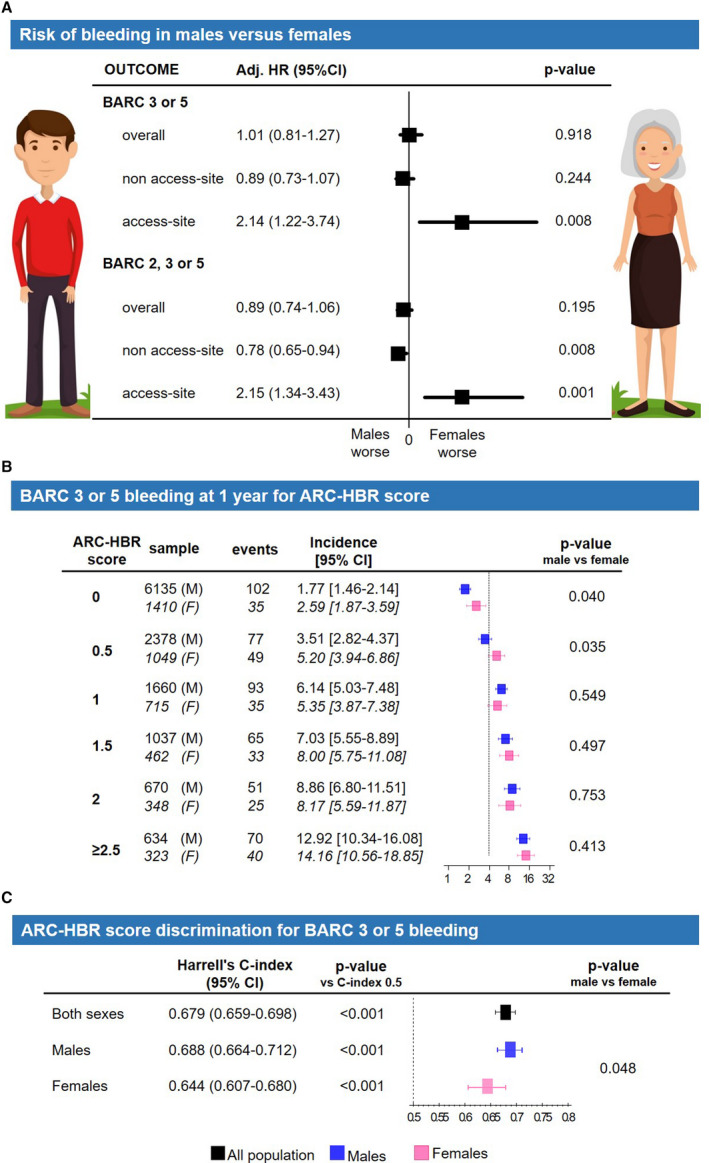
Background Female sex was not included among the high bleeding risk (HBR) criteria by the Academic Research Consortium (ARC) as it remains unclear whether it constitutes an HBR condition after percutaneous coronary intervention. We investigated whether female sex associates with HBR and assessed the performance of ARC HBR criteria separately in women and men. Methods and Results Among all consecutive patients undergoing percutaneous coronary intervention between 2009 and 2018, bleeding occurrences up to 1 year were prospectively collected and centrally adjudicated. All but one of the originally defined ARC HBR criteria were assessed, and the ARC HBR score generated accordingly. Among 16 821 patients, 25.6% were women. Compared with men, women were older and had lower creatinine clearance and hemoglobin values. After adjustment, female sex was independently associated with access-site (adjusted hazard ratio, 2.14; 95% CI, 1.22-3.74; =0.008) but not with overall or non-access-site 1-year Bleeding Academic Research Consortium 3 or 5 bleeding. This association remained consistent when the femoral but not the radial approach was chosen. The ARC HBR score discrimination, using the original criteria, was lower among women than men (c-index 0.644 versus 0.688; =0.048), whereas a revised ARC HBR score, in which age, creatinine clearance, and hemoglobin were modeled as continuous rather than dichotomized variables, performed similarly in both sexes. Conclusions Female sex is an independent predictor for access-site bleeding but not for overall bleeding events at 1 year after percutaneous coronary intervention. The ARC HBR framework shows an overall good performance in both sexes, yet is lower in women than men, attributable to dichotomization of age, creatinine clearance, and hemoglobin values, which are differently distributed between sexes. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02241291.
学术研究联合会(ARC)的高出血风险(HBR)标准中不包括女性性别,因为在经皮冠状动脉介入治疗后,其是否构成 HBR 条件仍不清楚。我们研究了女性性别是否与 HBR 相关,并分别评估了女性和男性中 ARC HBR 标准的表现。
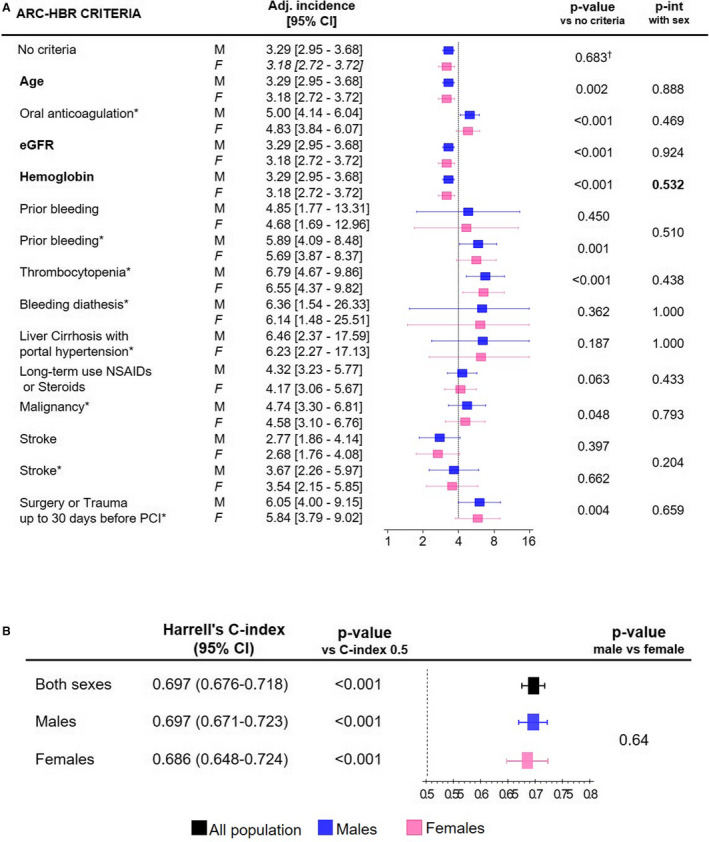
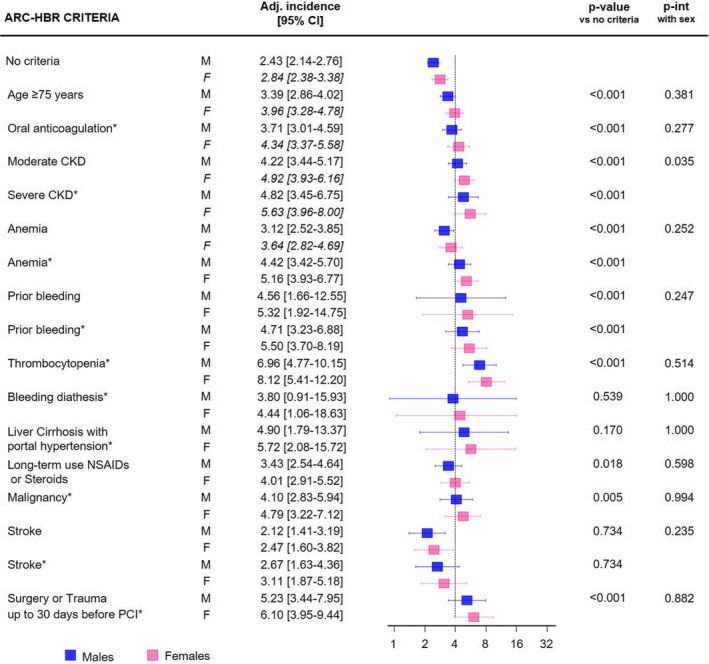
在 2009 年至 2018 年间连续接受经皮冠状动脉介入治疗的所有患者中,前瞻性地收集了 1 年内的出血事件,并进行了中心裁决。评估了除一个之外的所有最初定义的 ARC HBR 标准,并相应地生成了 ARC HBR 评分。在 16821 名患者中,25.6%为女性。与男性相比,女性年龄较大,肌酐清除率和血红蛋白值较低。调整后,女性性别与入路部位独立相关(调整后的危险比,2.14;95%置信区间,1.22-3.74;=0.008),但与总体或非入路部位 1 年 Bleeding Academic Research Consortium 3 或 5 出血无关。当选择股动脉而不是桡动脉途径时,这种相关性仍然一致。使用原始标准,ARC HBR 评分的区分度在女性中低于男性(c 指数 0.644 与 0.688;=0.048),而在将年龄、肌酐清除率和血红蛋白建模为连续变量而不是二分类变量的修正 ARC HBR 评分在两性中表现相似。
女性性别是经皮冠状动脉介入治疗 1 年后入路部位出血的独立预测因素,但不是总体出血事件的预测因素。ARC HBR 框架在两性中均表现出良好的总体性能,但在女性中低于男性,这归因于年龄、肌酐清除率和血红蛋白值的二分类,这些值在性别之间的分布不同。