Newlands Clinic, Newlands, Harare, Zimbabwe.
Institute of Social and Preventive Medicine, University of Bern, Bern, Switzerland.
PLoS One. 2021 Jun 9;16(6):e0253000. doi: 10.1371/journal.pone.0253000. eCollection 2021.
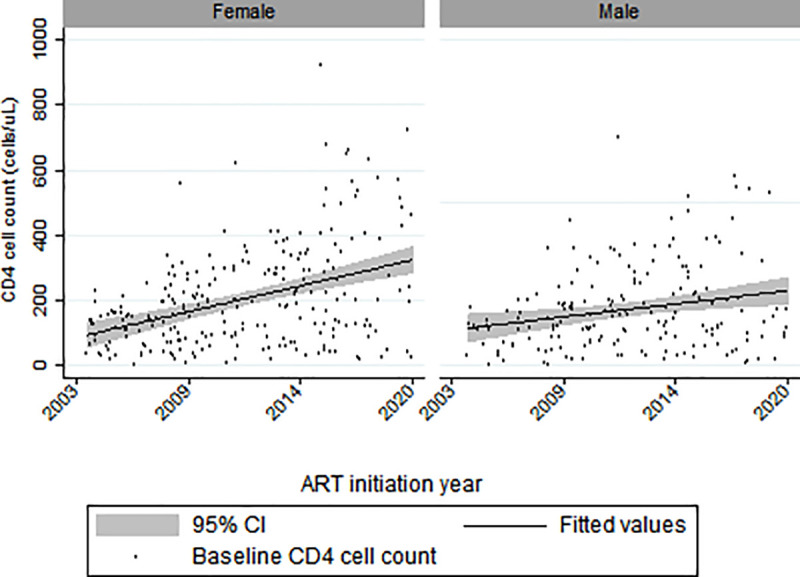
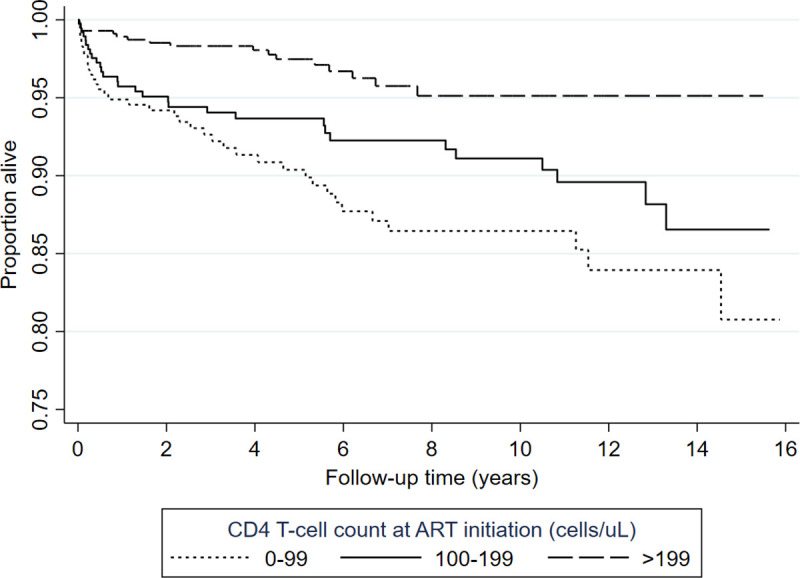
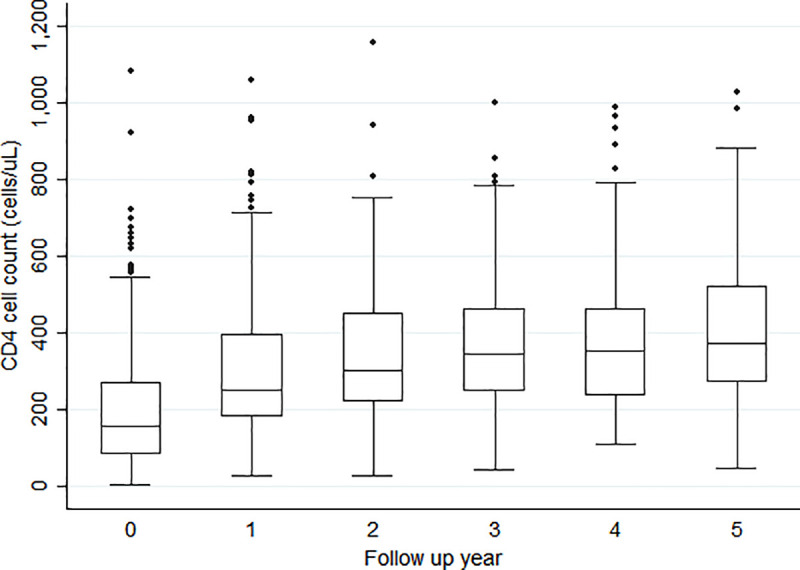
There is a growing number of older people living with HIV (OPLHIV). While a significant proportion of this population are adults growing into old age with HIV, there are also new infections among OPLHIV. There is a lack of data describing the outcomes of OPLHIV who commenced antiretroviral therapy (ART) after the age of 50 years in sub-Saharan Africa. We conducted a cohort study of patients who enrolled in care at Newlands Clinic in Harare, Zimbabwe, at ages ≥50 years between February 2004 and March 2020. We examined demographic characteristics, attrition, viral suppression, immunological and clinical outcomes. Specifically, we described prevalent and incident HIV-related communicable and non-communicable comorbidities. We calculated frequencies, medians, interquartile ranges (IQR), and proportions; and used Cox proportional hazards models to identify risk factors associated with death. We included 420 (57% female) who commenced ART and were followed up for a median of 5.6 years (IQR 2.4-9.9). Most of the men were married (n = 152/179, 85%) whereas women were mostly widowed (n = 125/241, 51.9%). Forty per cent (n = 167) had WHO stage 3 or 4 conditions at ART baseline. Hypertension prevalence was 15% (n = 61) at baseline, and a further 27% (n = 112) had incident hypertension during follow-up. During follow-up, 300 (71%) were retained in care, 88 (21%) died, 17 (4%) were lost to follow-up, and 15 (4%) were transferred out. Of those in care, 283 (94%) had viral loads <50 copies/ml, and 10 had viral loads >1000 copies/ml. Seven patients (1.7%) were switched to second line ART during follow-up and none were switched to third-line. Higher baseline CD4 T-cell counts were protective against mortality (p = 0.001) while male sex (aHR: 2.29, 95%CI: 1.21-4.33), being unmarried (aHR: 2.06, 95%CI: 1.13-3.78), and being unemployed (aHR: 2.01, 95%CI: 1.2-3.37) were independent independent risk factors of mortality. There was high retention in care and virologic suppression in this cohort of OPLHIV. Hypertension was a common comorbidity. Being unmarried or unemployed were significant predictors of mortality highlighting the importance of sociologic factors among OPLHIV, while better immune competence at ART commencement was protective against mortality.
越来越多的老年人携带艾滋病毒(OPLHIV)。尽管这一人群中的很大一部分是成年后感染艾滋病毒而进入老年的,但 OPLHIV 中也有新的感染。缺乏描述撒哈拉以南非洲地区 50 岁以上开始接受抗逆转录病毒治疗(ART)的 OPLHIV 结局的数据。我们对 2004 年 2 月至 2020 年 3 月在津巴布韦哈拉雷的 Newlands 诊所接受护理的年龄≥50 岁的患者进行了队列研究。我们检查了人口统计学特征、流失、病毒抑制、免疫和临床结局。具体来说,我们描述了现患和新发与 HIV 相关的传染性和非传染性合并症。我们计算了频率、中位数、四分位距(IQR)和比例;并使用 Cox 比例风险模型来确定与死亡相关的风险因素。我们纳入了 420 名(57%为女性)开始接受 ART 并随访中位数为 5.6 年(IQR 2.4-9.9)的患者。大多数男性已婚(n=152/179,85%),而女性大多丧偶(n=125/241,51.9%)。40%(n=167)在 ART 基线时患有世界卫生组织(WHO)第 3 或 4 期疾病。基线时高血压患病率为 15%(n=61),随访期间另有 27%(n=112)发生高血压。随访期间,300 名(71%)患者留在护理中,88 名(21%)死亡,17 名(4%)失访,15 名(4%)转院。在接受护理的患者中,283 名(94%)病毒载量<50 拷贝/ml,10 名病毒载量>1000 拷贝/ml。在随访期间,有 7 名(1.7%)患者转为二线 ART,没有患者转为三线。基线时较高的 CD4 T 细胞计数是死亡的保护因素(p=0.001),而男性(aHR:2.29,95%CI:1.21-4.33)、未婚(aHR:2.06,95%CI:1.13-3.78)和失业(aHR:2.01,95%CI:1.2-3.37)是死亡的独立危险因素。在这组 OPLHIV 中,患者的护理保留率和病毒抑制率均很高。高血压是一种常见的合并症。未婚或失业是死亡的显著预测因素,这突显了社会学因素在 OPLHIV 中的重要性,而在开始 ART 时更好的免疫能力是死亡的保护因素。