The Biomechanics Group, Department of Mechanical Engineering, Imperial College London, London, UK.
College of Engineering, Mathematics and Physical Sciences, University of Exeter, Exeter, UK.
Am J Sports Med. 2021 Jul;49(9):2351-2360. doi: 10.1177/03635465211020478. Epub 2021 Jun 14.
Little scientific evidence is available regarding the effect of knee joint line obliquity (JLO) before and after coronal realignment osteotomy.
Higher JLO would lead to abnormal relative position of the femur on the tibia, a shift of the joint contact areas, and elevated joint contact pressures.
Descriptive laboratory study.
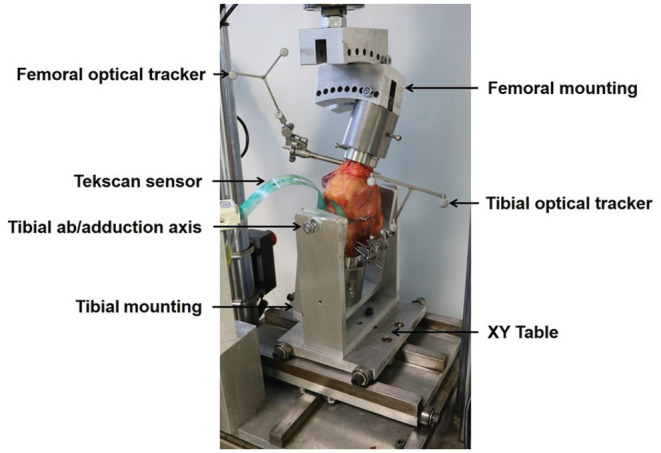
10 fresh-frozen human cadaveric knees (age, 59 ± 5 years) were axially loaded to 1500 N in a materials testing machine with the joint line tilted 0°, 4°, 8°, and 12° varus ("downhill" medially) and valgus, at 0° and 20° of knee flexion. The mechanical compression axis was aligned to the center of the tibial plateau. Contact pressure and contact area were recorded by pressure sensors inserted between the tibia and femur below the menisci. Changes in relative femoral and tibial position in the coronal plane were obtained by an optical tracking system.
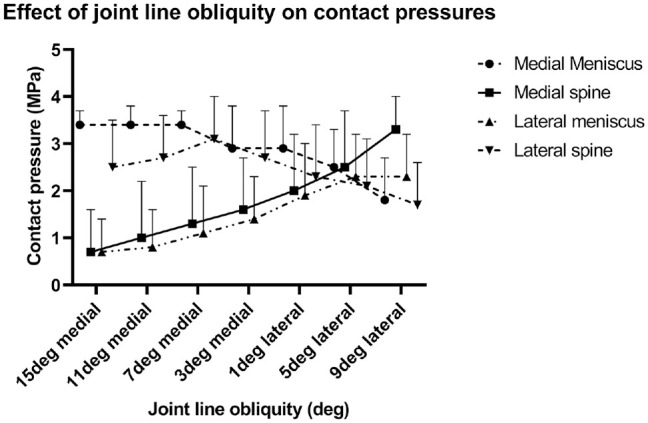
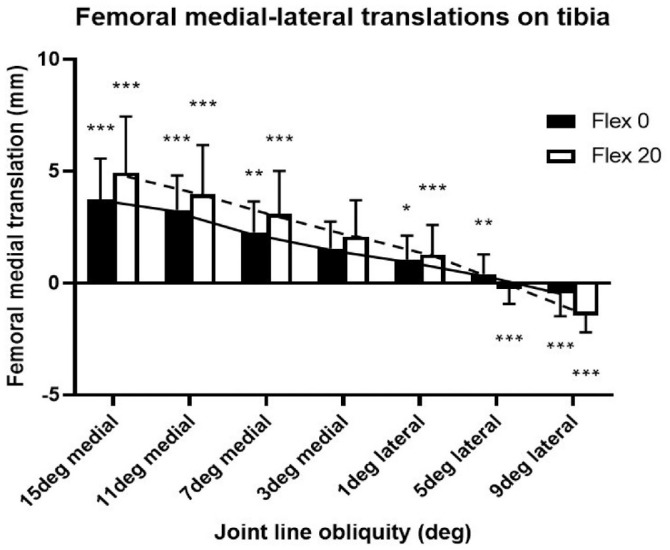
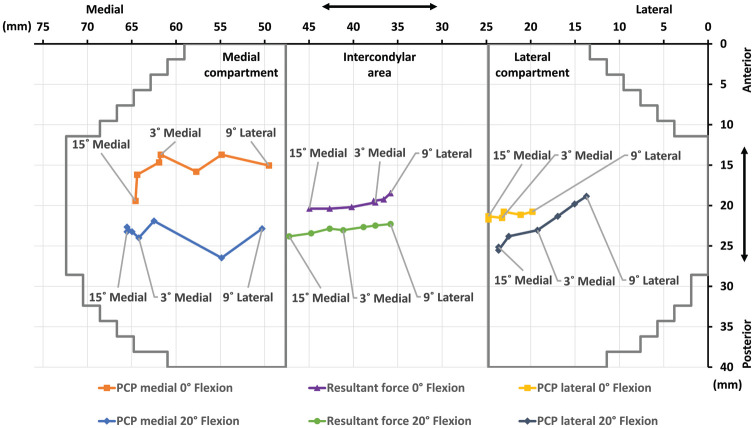
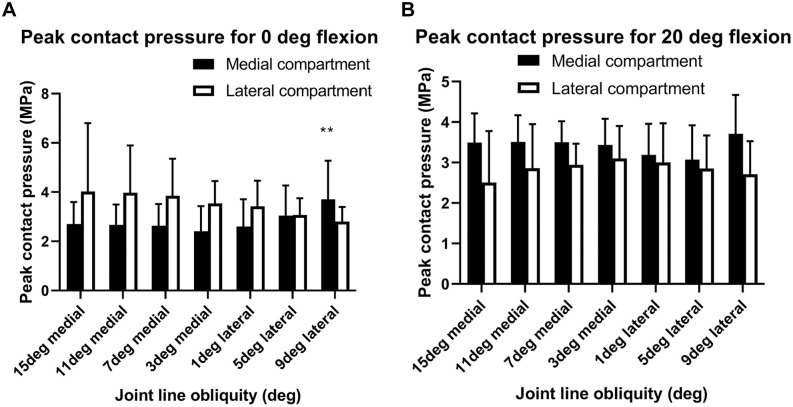
Both medial and lateral JLO caused significant tibiofemoral subluxation and pressure distribution changes. Medial (varus) JLO caused the femur to subluxate medially down the coronal slope of the tibial plateau, and vice versa for lateral (valgus) downslopes ( < .01), giving a 6-mm range of subluxation. The areas of peak pressure moved 12 mm and 8 mm across the medial and lateral condyles, onto the downhill meniscus and the "uphill" tibial spine. Changes in JLO had only small effects on maximum contact pressures.
A 4° change of JLO during load bearing caused significant mediolateral tibiofemoral subluxation. The femur slid down the slope of the tibial plateau to abut the tibial eminence and also to rest on the downhill meniscus. This caused large movements of the tibiofemoral contact pressures across each compartment.
These results provide important information for understanding the consequences of creating coronal JLO and for clinical practice in terms of osteotomy planning regarding the effect on JLO. This information provides guidance regarding the choice of single- or double-level osteotomy. Excessive JLO alteration may cause abnormal tibiofemoral joint articulation and chondral or meniscal loading.
关于冠状面矫正截骨术后膝关节对线(JLO)的前后变化对其影响的科学证据较少。
较高的 JLO 会导致股骨在胫骨上的相对位置异常,关节接触区域发生转移,关节接触压力升高。
描述性实验室研究。
在材料试验机上对 10 个新鲜冷冻的人体膝关节(年龄 59±5 岁)进行轴向加载至 1500N,关节线倾斜 0°、4°、8°和 12°(向内侧“下坡”)和外翻,在 0°和 20°的膝关节屈曲位。机械压缩轴与胫骨平台中心对齐。通过插入半月板下方胫骨和股骨之间的压力传感器记录接触压力和接触面积。通过光学跟踪系统获得冠状面中股骨和胫骨相对位置的变化。
内侧和外侧 JLO 均导致明显的胫骨股骨半脱位和压力分布变化。内侧(内翻)JLO 导致股骨在胫骨平台的冠状斜坡上向内侧半脱位,反之亦然,外侧(外翻)下坡时(<0.01),半脱位范围为 6mm。峰值压力区域在内外侧髁上移动了 12mm 和 8mm,移至下坡半月板和“上坡”胫骨棘上。JLO 的变化仅对最大接触压力有很小的影响。
在负重期间 JLO 发生 4°变化会导致明显的内外侧胫骨股骨半脱位。股骨在胫骨平台的斜坡上向下滑动,与胫骨嵴相接,并支撑在下坡半月板上。这导致了每个关节间的胫骨股骨接触压力的大幅度移动。
这些结果为理解冠状面 JLO 产生的后果以及在冠状面 JLO 影响方面的截骨术规划提供了重要信息,为临床实践提供了指导。这为单级或双级截骨术的选择提供了信息。过度改变 JLO 可能会导致异常的胫骨股骨关节关节面和软骨或半月板受力。