Inoue Koichi, Tanaka Nobuaki, Ikada Yusuke, Mizutani Akihiro, Yamamoto Kazuhiko, Matsuhira Hana, Harada Shinichi, Okada Masato, Iwakura Katsuomi, Fujii Kenshi
Sakurabashi Watanabe Hospital Osaka Japan.
Cardiovascular Division National Hospital Organization Osaka National Hospital Osaka Japan.
J Arrhythm. 2021 May 7;37(3):574-583. doi: 10.1002/joa3.12544. eCollection 2021 Jun.
Although usefulness of VISITAG SURPOINT (VS) on pulmonary vein isolation (PVI) in catheter ablation of atrial fibrillation has been reported, optimal VS thresholds can depend on the inter-tag distance (ITD) and vice versa. We validated the efficacy of PVI with lower target ITDs and VS values than in previous studies.
Retrospective review of consecutive patients (N = 100) with paroxysmal (n = 32) or persistent AF (n = 68) undergoing VS-guided ablation between 09/2018 and 08/2019 was conducted. All procedures were performed by two operators. Target VS values were 425 (anterior), 375 (posterior), and 325 (near the esophagus). Target ITD was 4 mm.
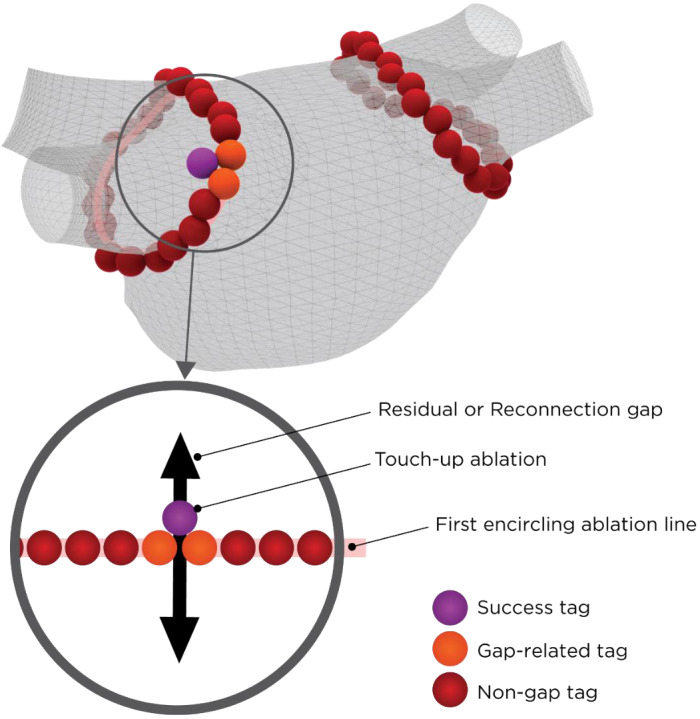
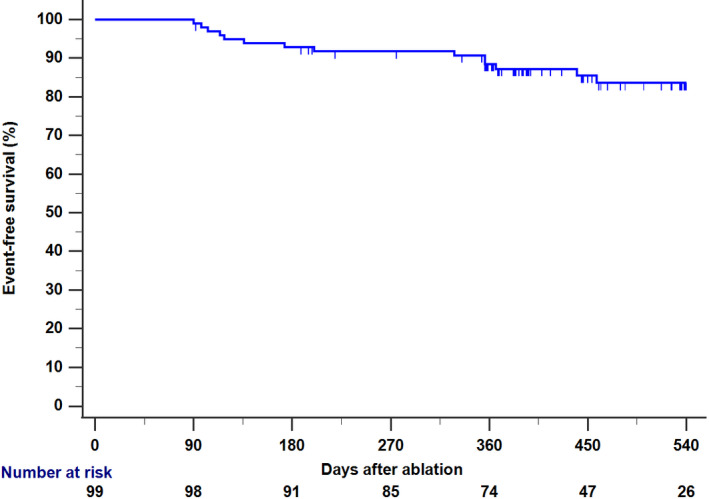
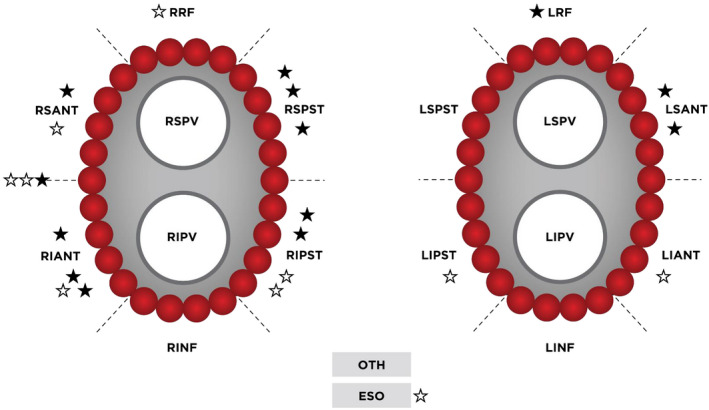
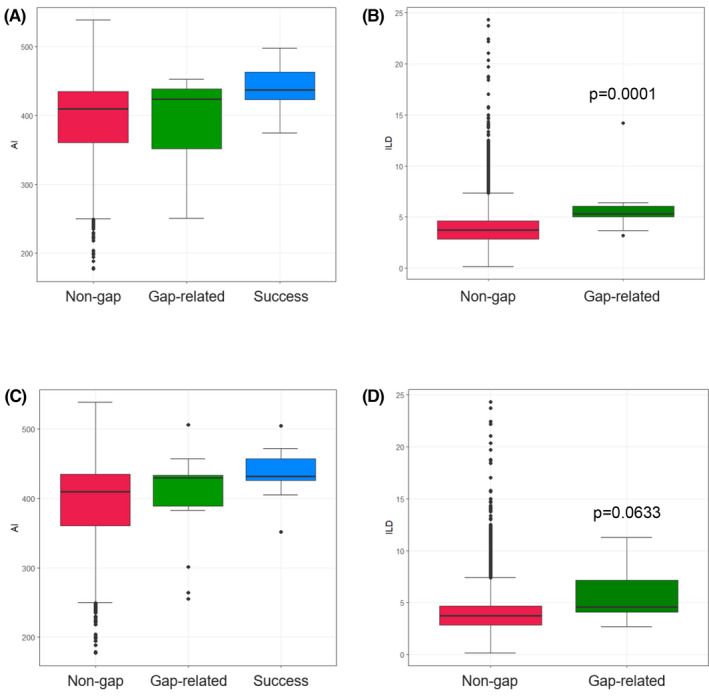
Acute PVI was achieved in all cases, however, 13 residual gaps in 12 patients were observed after initial encirclement (first pass isolation: 88%). Ten gaps due to spontaneous PV reconnections (PVR) were found in nine patients (9%). These 23 gaps had similar median VS (gap-related vs non-gap: 429 vs 410, = .4545) and power (36 vs 36W, = .4843), higher contact force (13.8 vs 11.0g, = .0061), and larger ITD (5.3 vs 3.7mm, < .001) when compared to the remaining tags. Only ITDs were independently associated with gap formation in multivariate analysis. One-year Kaplan-Meier freedom from any atrial arrhythmia was 87.2%. Eight patients received repeat ablation (8.1%) and of these, 6 (75%) were free from PVR.
Favorable rates of first pass isolation, acute PVR, and long-term procedure success were achieved using lower VS values than in previous reports. With a target VS value of 375-425, ITDs of 4 mm was sufficient for durable PVI.
尽管已有报道称VISITAG SURPOINT(VS)在房颤导管消融的肺静脉隔离(PVI)中具有有效性,但最佳VS阈值可能取决于标签间距(ITD),反之亦然。我们验证了与以往研究相比,采用更低目标ITD和VS值进行PVI的疗效。
对2018年9月至2019年8月期间接受VS引导下消融的100例连续性阵发性(n = 32)或持续性房颤(n = 68)患者进行回顾性分析。所有手术均由两名术者完成。目标VS值为425(前部)、375(后部)和325(食管附近)。目标ITD为4毫米。
所有病例均实现了急性PVI,但在初始环绕后,12例患者中观察到13处残留间隙(首次通过隔离:88%)。9例患者(9%)发现10处因肺静脉自发重新连接(PVR)导致的间隙。与其余标签相比,这23处间隙的VS中位数相似(间隙相关与非间隙:429对410,P = 0.4545)、功率相似(36对36W,P = 0.4843),接触力更高(13.8对11.0g,P = 0.0061),ITD更大(5.3对3.7mm,P < 0.001)。在多因素分析中,只有ITD与间隙形成独立相关。一年的无任何房性心律失常的Kaplan-Meier生存率为87.2%。8例患者接受了再次消融(8.1%),其中6例(75%)无PVR。
与以往报道相比,采用更低的VS值获得了良好的首次通过隔离率、急性PVR率和长期手术成功率。目标VS值为375 - 425时,4毫米的ITD足以实现持久的PVI。