Oncology Safety, Clinical Pharmacology and Safety Sciences, R&D, AstraZeneca, Cambridge, United Kingdom.
Bioscience, Oncology R&D, AstraZeneca, Cambridge, United Kingdom.
Mol Cancer Ther. 2021 Sep;20(9):1614-1626. doi: 10.1158/1535-7163.MCT-20-0502. Epub 2021 Jun 22.
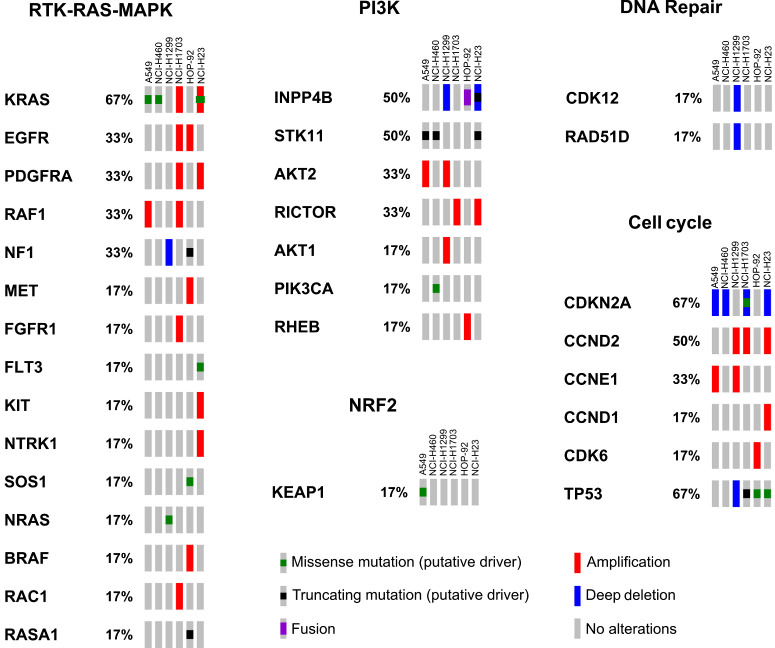
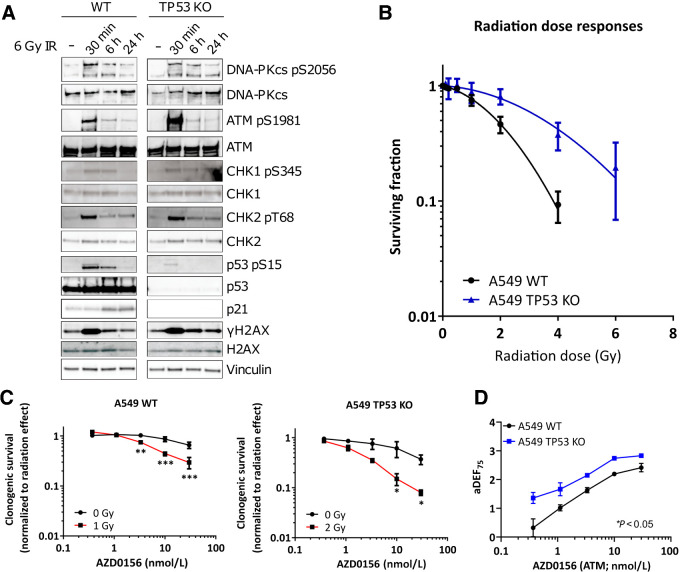
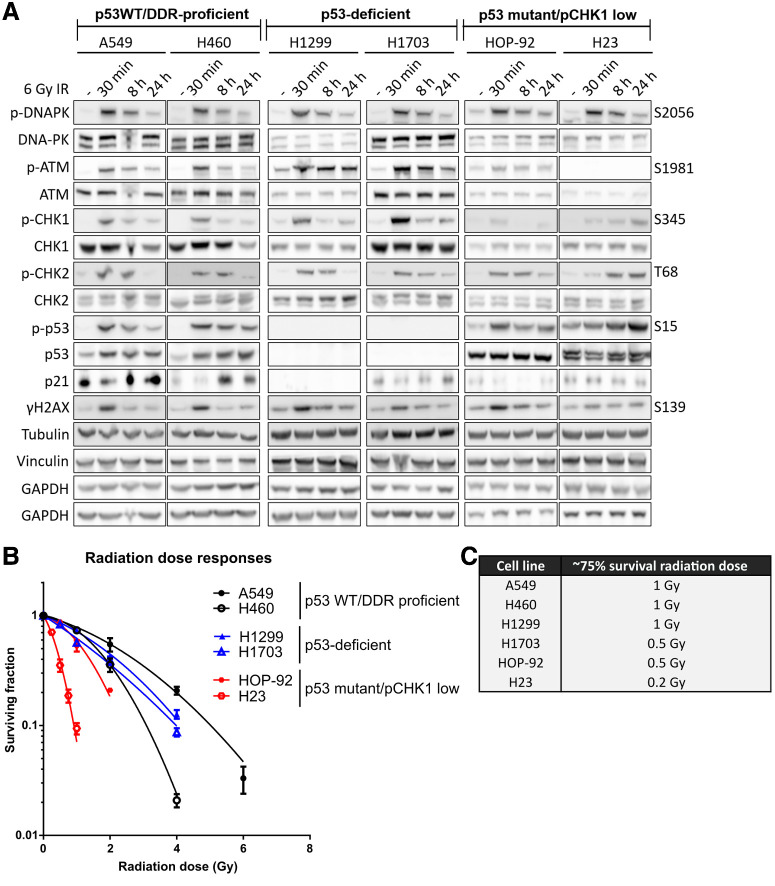
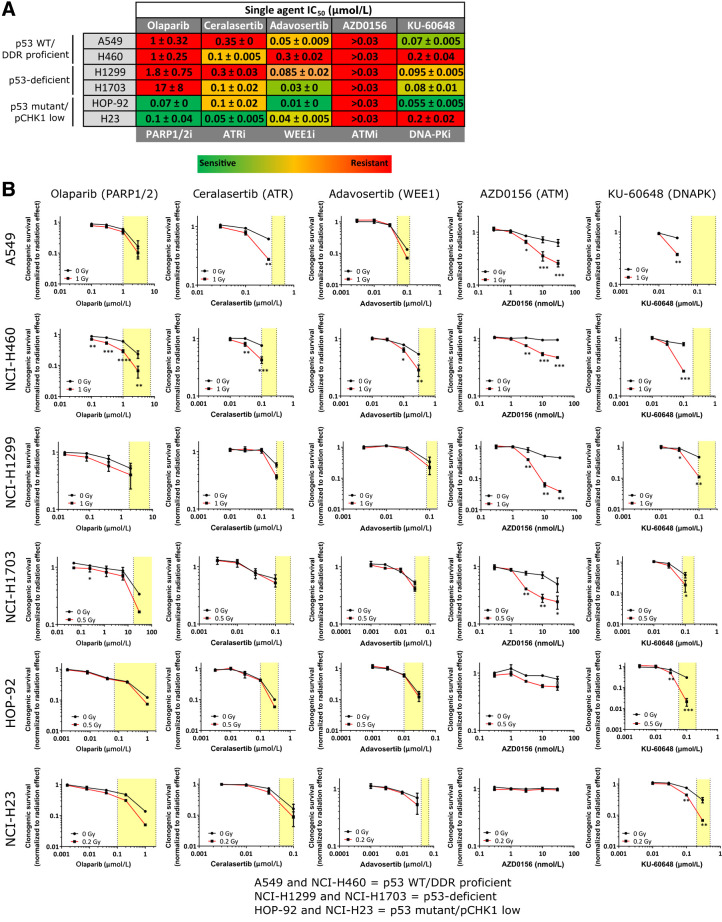
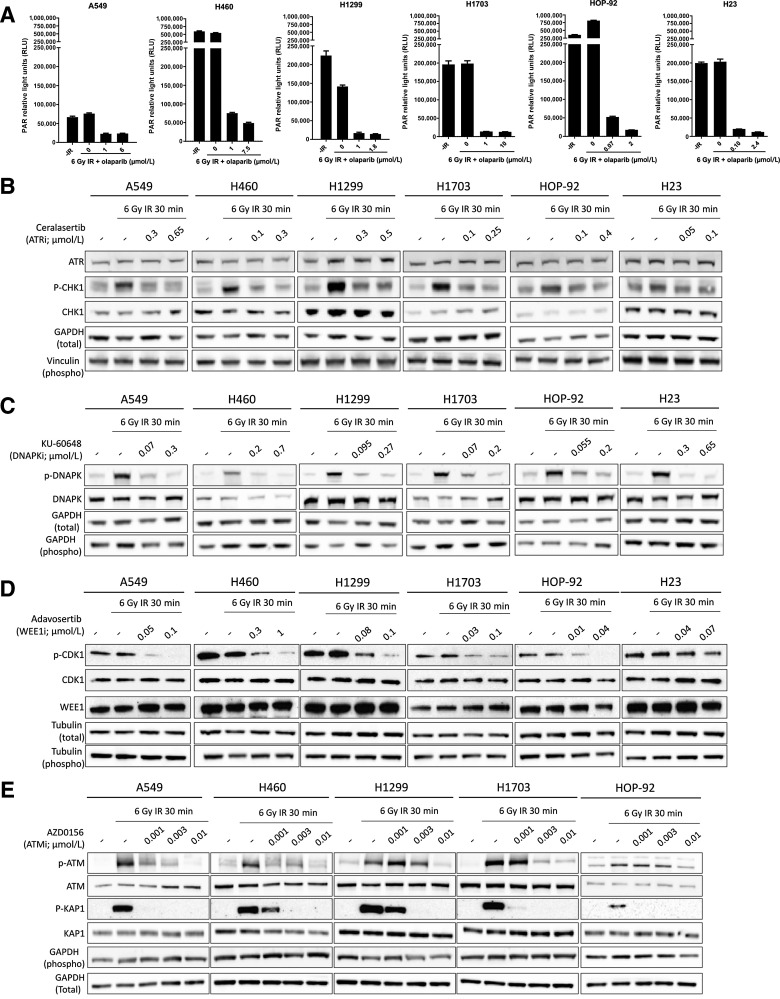
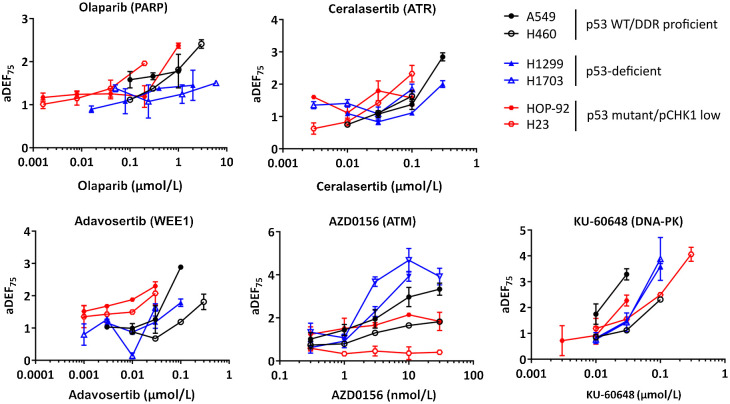
Radiotherapy is an effective anticancer treatment, but combinations with targeted agents that maximize efficacy while sparing normal tissue are needed. Here, we assess the radiopotentiation profiles of DNA damage response inhibitors (DDRi) olaparib (PARP1/2), ceralasertib (ATR), adavosertib (WEE1), AZD0156 (ATM), and KU-60648 (DNA-PK). We performed a radiotherapy combination screen and assessed how drug concentration and cellular DDR deficiencies influence the radiopotentiation ability of DDRi. We pre-selected six lung cancer cell lines with different genetic/signaling aberrations (including mutations in and ) and assessed multiple concentrations of DDRi in combination with a fixed radiotherapy dose by clonogenic assay. The effective concentration of DDRi in radiotherapy combinations is lower than that required for single-agent efficacy. This has the potential to be exploited further in the context of DDR deficiencies to increase therapeutic index and we demonstrate that low concentrations of AZD0156 preferentially sensitized p53-deficient cells. Moreover, testing multiple concentrations of DDRi in radiotherapy combinations indicated that olaparib, ceralasertib, and adavosertib have a desirable safety profile showing moderate increases in radiotherapy dose enhancement with increasing inhibitor concentration. Small increases in concentration of AZD0156 and particularly KU-60648, however, result in steep increases in dose enhancement. Radiopotentiation profiling can inform on effective drug doses required for radiosensitization in relation to biomarkers, providing an opportunity to increase therapeutic index. Moreover, multiple concentration testing demonstrates a relationship between drug concentration and radiotherapy effect that provides valuable insights that, with future validation, can guide dose-escalation strategies in clinical trials.
放射治疗是一种有效的抗癌治疗方法,但需要与靶向药物联合使用,以最大限度地提高疗效,同时保护正常组织。在这里,我们评估了 DNA 损伤反应抑制剂(DDRi)奥拉帕利(PARP1/2)、塞拉塞替布(ATR)、阿伐索替布(WEE1)、AZD0156(ATM)和 KU-60648(DNA-PK)的放射增敏作用。我们进行了放射治疗联合筛选,并评估了药物浓度和细胞 DDR 缺陷如何影响 DDRi 的放射增敏能力。我们预先选择了六种具有不同遗传/信号异常的肺癌细胞系(包括 和 突变),并通过集落形成试验评估了 DDRi 与固定放射剂量的多种浓度组合。放射治疗联合用药中 DDRi 的有效浓度低于单药疗效所需的浓度。这有可能在 DDR 缺陷的背景下进一步被利用,以增加治疗指数,我们证明低浓度的 AZD0156 优先敏化 p53 缺陷细胞。此外,在放射治疗联合用药中测试多种浓度的 DDRi 表明,奥拉帕利、塞拉塞替布和阿伐索替布具有理想的安全性特征,随着抑制剂浓度的增加,放射增敏作用适度增加。然而,AZD0156 和特别是 KU-60648 浓度的微小增加会导致放射增敏作用的剂量增强急剧增加。放射增敏作用分析可以为与生物标志物相关的放射增敏所需的有效药物剂量提供信息,从而有机会增加治疗指数。此外,多次浓度测试表明药物浓度与放射治疗效果之间存在关系,这提供了有价值的见解,如果在未来得到验证,可以指导临床试验中的剂量递增策略。