Department of Anesthesia and Critical Care, "Luigi Sacco" Hospital, ASST Fatebenefratelli-Sacco, Via G.B. Grassi, 74, 20157, Milan, Italy.
Department of Anesthesia, Critical Care, and Pain Medicine, Massachusetts General Hospital, Boston, MA, USA.
J Nephrol. 2022 Jan;35(1):99-111. doi: 10.1007/s40620-021-01100-3. Epub 2021 Jun 25.
Acute kidney injury (AKI) in Covid-19 patients admitted to the intensive care unit (ICU) is common, and its severity may be associated with unfavorable outcomes. Severe Covid-19 fulfills the diagnostic criteria for acute respiratory distress syndrome (ARDS); however, it is unclear whether there is any relationship between ventilatory management and AKI development in Covid-19 ICU patients.
To describe the clinical course and outcomes of Covid-19 ICU patients, focusing on ventilatory management and factors associated with AKI development.
Single-center, retrospective observational study, which assessed AKI incidence in Covid-19 ICU patients divided by positive end expiratory pressure (PEEP) tertiles, with median levels of 9.6 (low), 12.0 (medium), and 14.7 cmHO (high-PEEP).
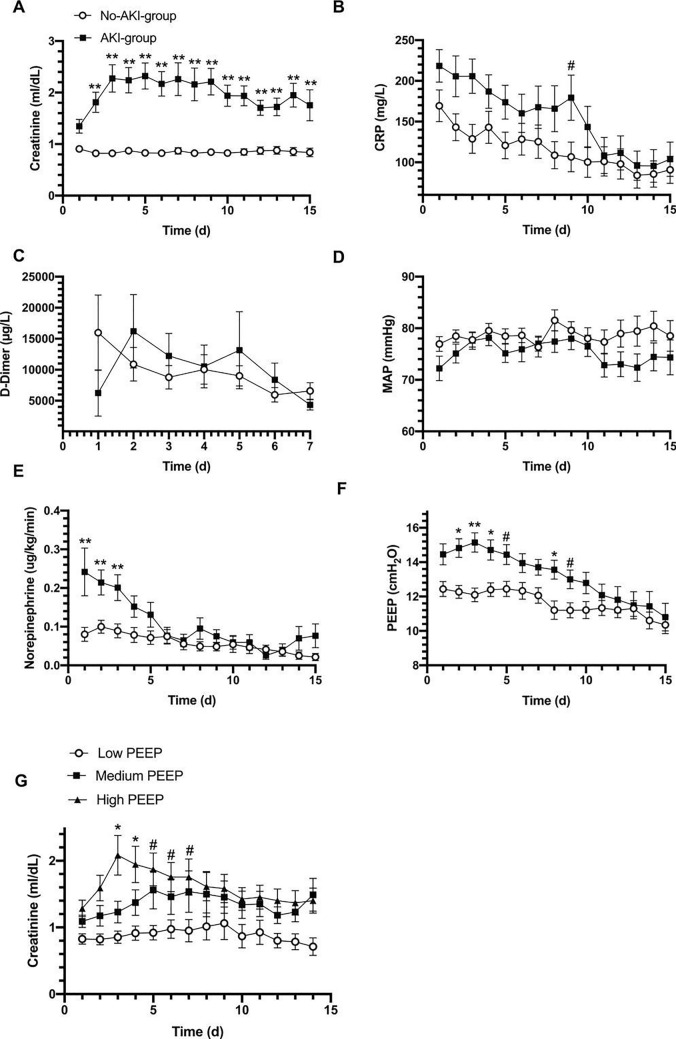
Overall mortality was 51.5%. AKI (KDIGO stage 2 or 3) occurred in 38% of 101 patients. Among the AKI patients, 19 (53%) required continuous renal replacement therapy (CRRT). In AKI patients, mortality was significantly higher versus non-AKI (81% vs. 33%, p < 0.0001). The incidence of AKI in low-, medium-, or high-PEEP patients were 16%, 38%, and 59%, respectively (p = 0.002). In a multivariate analysis, high-PEEP patients showed a higher risk of developing AKI than low-PEEP patients (OR = 4.96 [1.1-21.9] 95% CI p < 0.05). ICU mortality rate was higher in high-PEEP patients, compared to medium-PEEP or low-PEEP patients (69% vs. 44% and 42%, respectively; p = 0.057).
The use of high PEEP in Covid-19 ICU patients is associated with a fivefold higher risk of AKI, leading to higher mortality. The cause and effect relationship needs further analysis.
在入住重症监护病房(ICU)的新冠患者中,急性肾损伤(AKI)很常见,其严重程度可能与不良预后相关。重症新冠符合急性呼吸窘迫综合征(ARDS)的诊断标准;然而,在新冠 ICU 患者中,通气管理与 AKI 发展之间是否存在任何关系尚不清楚。
描述新冠 ICU 患者的临床过程和结局,重点关注通气管理和与 AKI 发展相关的因素。
这是一项单中心、回顾性观察性研究,评估了按呼气末正压(PEEP)三分位划分的新冠 ICU 患者的 AKI 发生率,中位 PEEP 水平分别为 9.6(低)、12.0(中)和 14.7 cmH2O(高 PEEP)。
总体死亡率为 51.5%。101 例患者中 AKI(KDIGO 分期 2 或 3 期)发生率为 38%。在 AKI 患者中,有 19 例(53%)需要持续肾脏替代治疗(CRRT)。与非 AKI 患者相比,AKI 患者的死亡率显著更高(81% vs. 33%,p<0.0001)。低、中、高 PEEP 患者的 AKI 发生率分别为 16%、38%和 59%(p=0.002)。多变量分析显示,与低 PEEP 患者相比,高 PEEP 患者发生 AKI 的风险更高(OR=4.96[1.1-21.9]95%CI p<0.05)。与中 PEEP 或低 PEEP 患者相比,高 PEEP 患者的 ICU 死亡率更高(分别为 69%、44%和 42%;p=0.057)。
在新冠 ICU 患者中使用高 PEEP 与 AKI 风险增加五倍相关,导致死亡率更高。因果关系需要进一步分析。