Clark David, Matheson Kara, West Benjamin, Vinson Amanda, West Kenneth, Jain Arsh, Rockwood Kenneth, Tennankore Karthik
Department of Medicine, Dalhousie University, Halifax, NS, Canada.
Department of Engineering, Dalhousie University, Halifax, NS, Canada.
Can J Kidney Health Dis. 2021 Jun 10;8:20543581211023330. doi: 10.1177/20543581211023330. eCollection 2021.
Frailty is associated with hospitalization and mortality among dialysis patients. To now, few studies have considered the degree of frailty as a predictor of hospitalization.
We evaluated whether was associated with hospitalization after dialysis initiation.
Retrolective cohort study.
Nova Scotia, Canada.
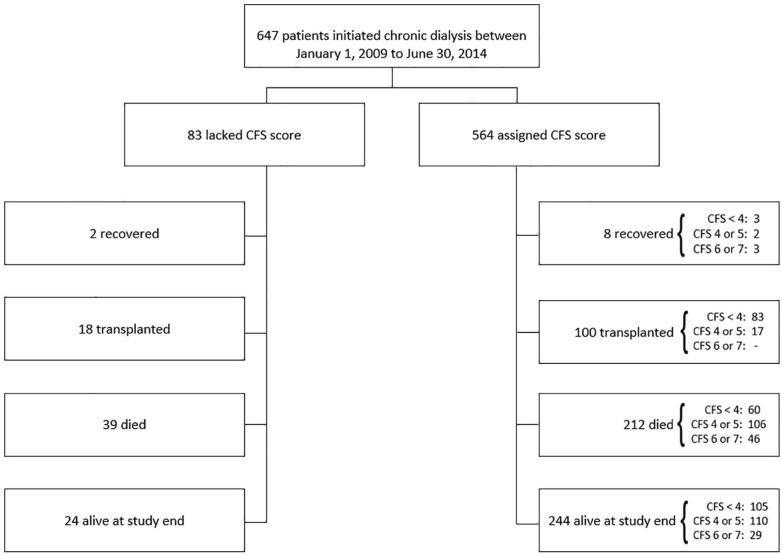
Consecutive adult, chronic dialysis patients who initiated dialysis from January 1, 2009 to June 30, 2014, (last follow-up June, 2015).
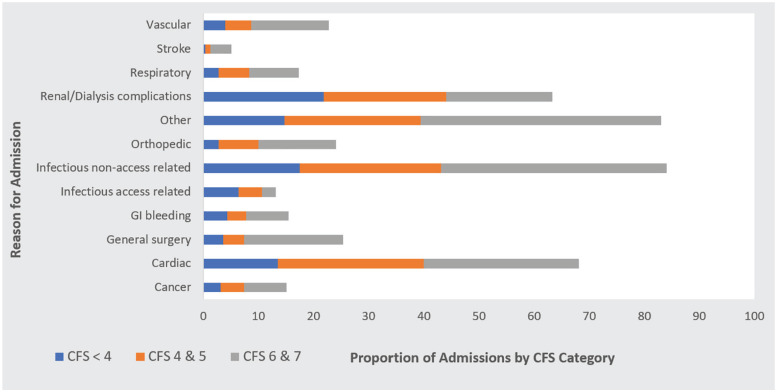
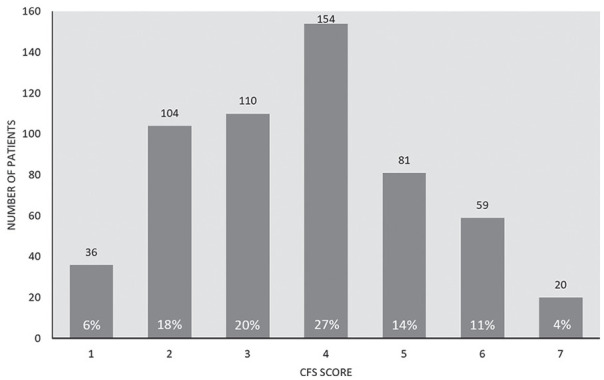
Frailty Severity, as determined by the 7-point Clinical Frailty Scale (CFS, ranging from 1 = very fit to 7 = severely frail), was measured at dialysis initiation and treated as continuous and in categories (CFS scores of 1-3, 4/5, and 6/7). Hospitalization was characterized by cumulative time admitted to hospital (proportion of days admitted/time at risk) and by the joint risk of hospitalization and death. Time at risk included time in hospital after dialysis initiation and patients were followed until transplantation or death.
Of 647 patients (mean age: 62 ± 15), 564 (87%) had CFS scores. The mean CFS score was 4 ("corresponding to "vulnerable") ± 2 ("well" to "moderately frail"). In an adjusted negative binomial regression model, moderate-severely frail patients (CFS 6/7) had a >2-fold increased risk of cumulative time admitted to hospital compared to the lowest CFS category (IRR = 2.18, 95% confidence interval [CI] = 1.31-3.63). In the joint model, moderate-severely frail patients had a 61% increase in the relative hazard for hospitalization (hazard ratio [HR] = 1.61, 95% CI = 1.29-2.02) and a 93% increase in the relative hazard for death compared to the lowest CFS category (HR = 1.93, 95% CI = 1.16-3.22).
Potential unknown confounders may have affected the association between frailty severity and hospitalization given observational study design. The CFS is subjective and different clinicians may grade frailty severity differently or misclassify patients on the basis of limited availability.
Among incident dialysis patients, a higher frailty severity as defined by the CFS is associated with both an increased risk of cumulative time admitted to hospital and joint risk of hospitalization and death.
衰弱与透析患者的住院率及死亡率相关。到目前为止,很少有研究将衰弱程度视为住院的预测指标。
我们评估了[此处原文似乎有缺失内容]在透析开始后是否与住院相关。
回顾性队列研究。
加拿大新斯科舍省。
2009年1月1日至2014年6月30日开始透析的连续成年慢性透析患者(最后随访时间为2015年6月)。
通过7分临床衰弱量表(CFS,范围从1 = 非常健康到7 = 严重衰弱)确定的衰弱严重程度在透析开始时进行测量,并作为连续变量和分类变量处理(CFS评分为1 - 3、4/5和6/7)。住院情况通过累计住院时间(住院天数比例/风险时间)以及住院和死亡的联合风险来表征。风险时间包括透析开始后的住院时间,患者随访至移植或死亡。
647例患者(平均年龄:62±15岁)中,564例(87%)有CFS评分。CFS平均评分为4(“对应于‘脆弱’”)±2(“健康”至“中度衰弱”)。在调整后的负二项回归模型中,与最低CFS类别相比,中度至重度衰弱患者(CFS 6/7)累计住院时间的风险增加超过2倍(发病率比[IRR]=2.18,95%置信区间[CI]=1.31 - 3.63)。在联合模型中,与最低CFS类别相比,中度至重度衰弱患者住院的相对风险增加61%(风险比[HR]=1.61,95%CI = 1.29 - 2.02),死亡的相对风险增加93%(HR = 1.93,95%CI = 1.16 - 3.22)。
鉴于观察性研究设计,潜在的未知混杂因素可能影响了衰弱严重程度与住院之间的关联。CFS是主观的,不同的临床医生可能对衰弱严重程度分级不同,或者基于有限的信息对患者进行错误分类。
在新接受透析的患者中,CFS定义的较高衰弱严重程度与累计住院时间增加以及住院和死亡的联合风险相关。