Medical Department II, LMU Hospital Munich, Marchioninistr. 15, 81377, Munich, Germany.
Medical Department III, LMU Hospital Munich, Marchioninistr. 15, 81377, Munich, Germany.
BMC Anesthesiol. 2021 Jun 28;21(1):178. doi: 10.1186/s12871-021-01396-5.
Point-of-care lung ultrasound (LU) is an established tool in the first assessment of patients with coronavirus disease (COVID-19). Purpose of this study was to evaluate the value of lung ultrasound in COVID-19 intensive care unit (ICU) patients in predicting clinical course and outcome.
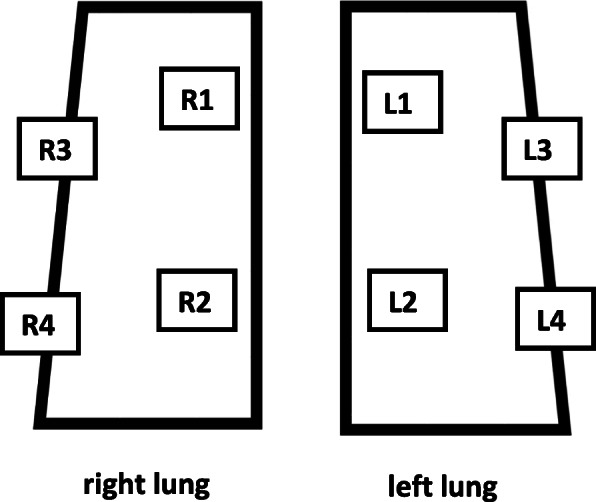
We analyzed lung ultrasound score (LUS) of all COVID-19 patients admitted from March 2020 to December 2020 to the Internal Intensive Care Unit, Ludwig-Maximilians-University (LMU) of Munich. LU was performed according to a standardized protocol at ICU admission and in case of clinical deterioration with the need for intubation. A normal lung scores 0 points, the worst LUS has 24 points. Patients were stratified in a low (0-12 points) and a high (13-24 points) lung ultrasound score group.
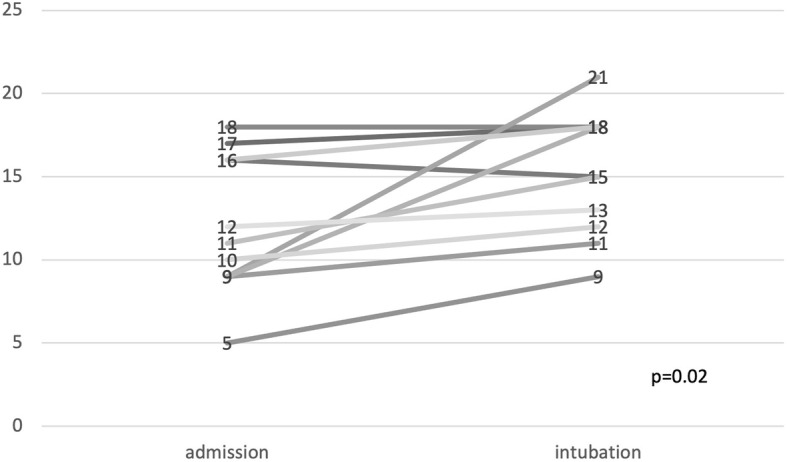
The study included 42 patients, 69% of them male. The most common comorbidities were hypertension (81%) and obesity (57%). The values of pH (7.42 ± 0.09 vs 7.35 ± 0.1; p = 0.047) and pO (107 [80-130] vs 80 [66-93] mmHg; p = 0.034) were significantly reduced in patients of the high LUS group. Furthermore, the duration of ventilation (12.5 [8.3-25] vs 36.5 [9.8-70] days; p = 0.029) was significantly prolonged in this group. Patchy subpleural thickening (n = 38; 90.5%) and subpleural consolidations (n = 23; 54.8%) were present in most patients. Pleural effusion was rare (n = 4; 9.5%). The median total LUS was 11.9 ± 3.9 points. In case of clinical deterioration with the need for intubation, LUS worsened significantly compared to baseline LU. Twelve patients died during the ICU stay (29%). There was no difference in survival in both LUS groups (75% vs 66.7%, p = 0.559).
LU can be a useful monitoring tool to predict clinical course but not outcome of COVID-19 ICU patients and can early recognize possible deteriorations.
床边肺部超声(Lung Ultrasound,LU)是评估新型冠状病毒肺炎(Coronavirus Disease 2019,COVID-19)患者的重要工具。本研究旨在评估 COVID-19 重症监护病房(Intensive Care Unit,ICU)患者肺部超声评分(Lung Ultrasound Score,LUS)对临床病程和预后的预测价值。
我们分析了 2020 年 3 月至 2020 年 12 月期间入住慕尼黑路德维希-马克西米利安大学(Ludwig-Maximilians-University,LMU)内科 ICU 的所有 COVID-19 患者的肺部超声评分。肺部超声检查按照标准方案进行,在 ICU 入院时以及出现临床恶化需要插管时进行。正常肺部评分 0 分,最差肺部超声评分 24 分。患者分为低(0-12 分)和高(13-24 分)肺部超声评分组。
本研究共纳入 42 例患者,其中 69%为男性。最常见的合并症为高血压(81%)和肥胖(57%)。高肺部超声评分组的 pH 值(7.42±0.09 比 7.35±0.1;p=0.047)和 pO2(107[80-130]比 80[66-93]mmHg;p=0.034)明显降低。此外,该组患者的通气时间(12.5[8.3-25]比 36.5[9.8-70]天;p=0.029)明显延长。大多数患者存在斑片状胸膜下增厚(n=38;90.5%)和胸膜下实变(n=23;54.8%)。胸腔积液少见(n=4;9.5%)。总肺部超声评分中位数为 11.9±3.9 分。在出现临床恶化需要插管的情况下,与基线肺部超声比较,肺部超声评分明显恶化。12 例患者在 ICU 期间死亡(29%)。两组患者的生存率无差异(75%比 66.7%,p=0.559)。
肺部超声可作为一种有用的监测工具,预测 COVID-19 ICU 患者的临床病程,但不能预测预后,并能早期识别可能的恶化。