Department of Orthopaedics, Balgrist University Hospital, University of Zurich, Forchstrasse 340, 8008, Zurich, Switzerland.
Sci Rep. 2021 Jun 28;11(1):13391. doi: 10.1038/s41598-021-90574-z.
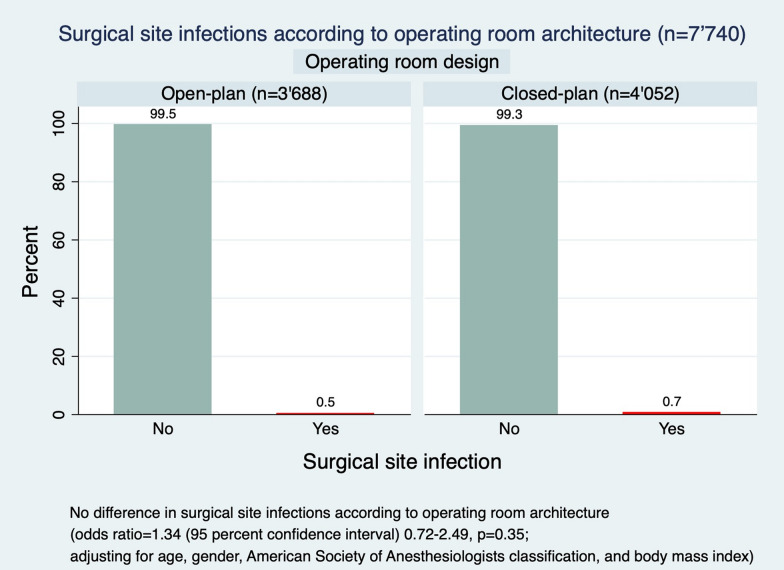
Surgical site infection (SSI) may cause a substantial burden for patients and healthcare systems. A potential risk of different architectures of the operating room for SSI is yet unknown and was subject of this study. This observational cohort study was performed in a university hospital and evaluated patients, who underwent a broad spectrum of orthopedic surgeries in 2016 (open-plan operating room architecture) versus (vs) 2017 (closed-plan operating room architecture). Patients, who underwent surgery in the transition time period from the open-plan to the closed-plan operating room architecture and those, who were treated e.g. for osteomyelitis as index procedure were excluded. The primary outcome was revision surgery for early SSI within 30 (superficial) or 90 (deep or organ/space) days of surgery. Age, gender, American society of anesthesiologists (ASA) classification, and the body mass index (BMI) were considered as potential interacting factors in a logistic regression analysis. The incidence of revisions for SSI was 0.6 percent (%) (n = 45) in the 7'740 included surgical cases (mean age of 52 (standard deviation (SD) 19) years; n = 3'835 (50%) females). There was no difference in incidences of revision for SSI in the open- vs closed-plan operating room architecture (0.5% vs 0.7%; adjusted odds ratio (OR) = 1.34 (95% confidence interval (CI) 0.72-2.49, P = 0.35)). Age and gender were not a risk factor for revision for SSI. However, ASA classification and BMI were identified as risk factors for the incidence of revision for SSI (OR = 1.92 (95% CI 1.16- 3.18, P = 0.01) and OR = 1.05 (95% CI 1.00-1.11, P = 0.05)). The overall incidence of revisions for early SSI after a broad spectrum of orthopedic surgeries was relatively low (0.6%) and independent from the operating room architecture. An increase in ASA classification and possibly BMI, however, were identified as independent risk factors for revision for SSI.
手术部位感染(SSI)可能给患者和医疗系统带来巨大负担。不同手术室结构对 SSI 的潜在风险尚不清楚,这也是本研究的主题。本观察性队列研究在一所大学医院进行,评估了 2016 年(开放式手术室结构)和 2017 年(封闭式手术室结构)期间接受广泛骨科手术的患者。排除了在开放式到封闭式手术室结构过渡期间接受手术的患者,以及作为索引手术接受治疗(例如骨髓炎)的患者。主要结局是术后 30 天(浅表)或 90 天(深部或器官/间隙)内因早期 SSI 而进行的翻修手术。年龄、性别、美国麻醉医师协会(ASA)分类和体重指数(BMI)被视为逻辑回归分析中的潜在交互因素。7740 例手术中,SSI 翻修的发生率为 0.6%(n=45)(平均年龄 52 岁(标准差 19 岁);n=3835 例(50%)女性)。开放式与封闭式手术室结构的 SSI 翻修发生率无差异(0.5%比 0.7%;调整后比值比(OR)=1.34(95%置信区间(CI)0.72-2.49,P=0.35))。年龄和性别不是 SSI 翻修的危险因素。然而,ASA 分类和 BMI 被确定为 SSI 翻修发生率的危险因素(OR=1.92(95%CI 1.16-3.18,P=0.01)和 OR=1.05(95%CI 1.00-1.11,P=0.05))。广泛骨科手术后早期 SSI 翻修的总体发生率相对较低(0.6%),与手术室结构无关。然而,ASA 分类和 BMI 增加被确定为 SSI 翻修的独立危险因素。