Li Xun, Yan Haipeng, Xiao Zhenghui, Zhang Xinping, Huang Jiaotian, Xiang Shi-Ting, Zheng Mincui, Yao Zhenya, Zang Ping, Zhu Desheng, Li Liping, Lu Xiulan
Pediatrics Research Institute of Hunan Province, Hunan Children's Hospital, Changsha, China.
Department of Pediatric Intensive Care Unit, Hunan Children's Hospital, Changsha, China.
Front Pediatr. 2021 Jun 17;9:692849. doi: 10.3389/fped.2021.692849. eCollection 2021.
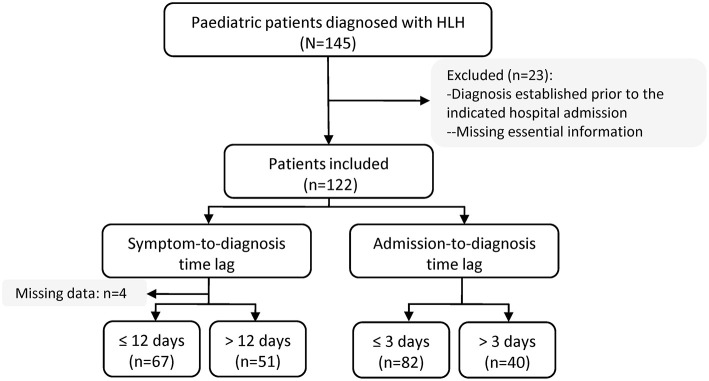
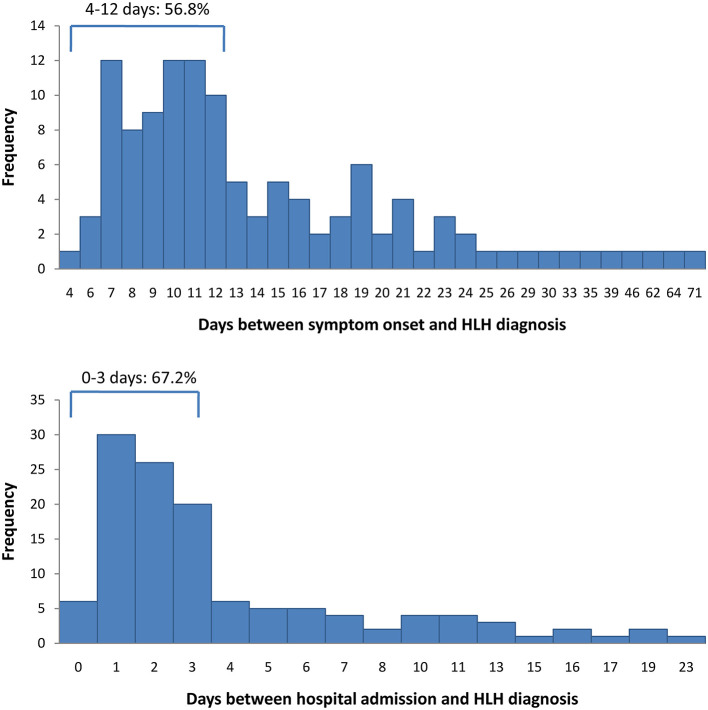
The difficulties and challenges of applying the HLH-2004 diagnostic criteria to early identification and diagnosis of haemophagocytic lymphohistiocytosis have been fully addressed in previous studies. However, the distribution of the diagnostic time lag of haemophagocytic lymphohistiocytosis and related patient characteristics remain unclear. This study investigated the time lags between symptom onset and diagnosis and between hospital admission and diagnosis among pediatric patients with haemophagocytic lymphohistiocytosis, and identified factors that associated with a shorter or longer diagnostic time lag. The cohort of patients with haemophagocytic lymphohistiocytosis was drawn from a tertiary children's hospital and consisted of 122 pediatric patients. The distributions of symptom-to-diagnosis and admission-to-diagnosis time lags were assessed. Clinical characteristics within 48 h of admission and the fulfillment of HLH-2004 diagnostic criteria were compared among admission-to-diagnosis time lag categories. Logistic regression analyses were conducted to identify factors associated with an admission-to-diagnosis time lag >3 days. The median interval from first symptom onset to HLH diagnosis was 12 days (range 4-71 days) and the median interval from hospital admission to HLH diagnosis was 2 days (range 0-23 days). The following factors were negatively associated with admission-to-diagnosis > 3 days: Epstein-Barr virus infection; admission through pediatric intensive care unit; diagnosis established without NK-cell activity and soluble CD25 tests; the performance of all readily available diagnostic tests for HLH (within 48 and 72 h); concurrent fever, splenomegaly, and cytopenias within 48 h; hemophagocytosis, hypertriglyceridemia and/or hypofibrinogenemia within 48 h; and elevated ferritin, total bilirubin, alanine aminotransferase, and prothrombin time within 48 h. Our findings suggest that performance of adequate diagnostic tests for HLH is essential for early diagnosis of HLH. Once suspected, immediate and adequate diagnostic tests for HLH should be arranged for PICU patients. Improvements in diagnostic procedures and monitoring plans are needed to promote early diagnosis of HLH.
先前的研究已充分探讨了应用HLH - 2004诊断标准对噬血细胞性淋巴组织细胞增生症进行早期识别和诊断时所面临的困难与挑战。然而,噬血细胞性淋巴组织细胞增生症的诊断时间间隔分布以及相关患者特征仍不明确。本研究调查了噬血细胞性淋巴组织细胞增生症儿科患者从症状出现到诊断以及从入院到诊断的时间间隔,并确定了与诊断时间间隔较短或较长相关的因素。噬血细胞性淋巴组织细胞增生症患者队列来自一家三级儿童医院,由122名儿科患者组成。评估了从症状到诊断以及从入院到诊断的时间间隔分布。比较了入院48小时内的临床特征以及HLH - 2004诊断标准的满足情况在不同入院到诊断时间间隔类别之间的差异。进行逻辑回归分析以确定与入院到诊断时间间隔>3天相关的因素。从首次症状出现到HLH诊断的中位间隔时间为12天(范围4 - 71天),从入院到HLH诊断的中位间隔时间为2天(范围0 - 23天)。以下因素与入院到诊断>3天呈负相关:爱泼斯坦 - 巴尔病毒感染;通过儿科重症监护病房入院;在未进行自然杀伤细胞活性和可溶性CD25检测的情况下确诊;在48小时和72小时内完成所有可用的HLH诊断检测;入院48小时内同时出现发热、脾肿大和血细胞减少;入院48小时内出现噬血细胞现象、高甘油三酯血症和/或低纤维蛋白原血症;以及入院48小时内铁蛋白、总胆红素、丙氨酸氨基转移酶和凝血酶原时间升高。我们的研究结果表明,进行充分的HLH诊断检测对于HLH的早期诊断至关重要。一旦怀疑,应立即为儿科重症监护病房患者安排充分的HLH诊断检测。需要改进诊断程序和监测计划以促进HLH的早期诊断。