Eurotransplant Reference Laboratory, Leiden University Medical Center, Leiden, Netherlands.
Front Immunol. 2021 Jun 25;12:687254. doi: 10.3389/fimmu.2021.687254. eCollection 2021.
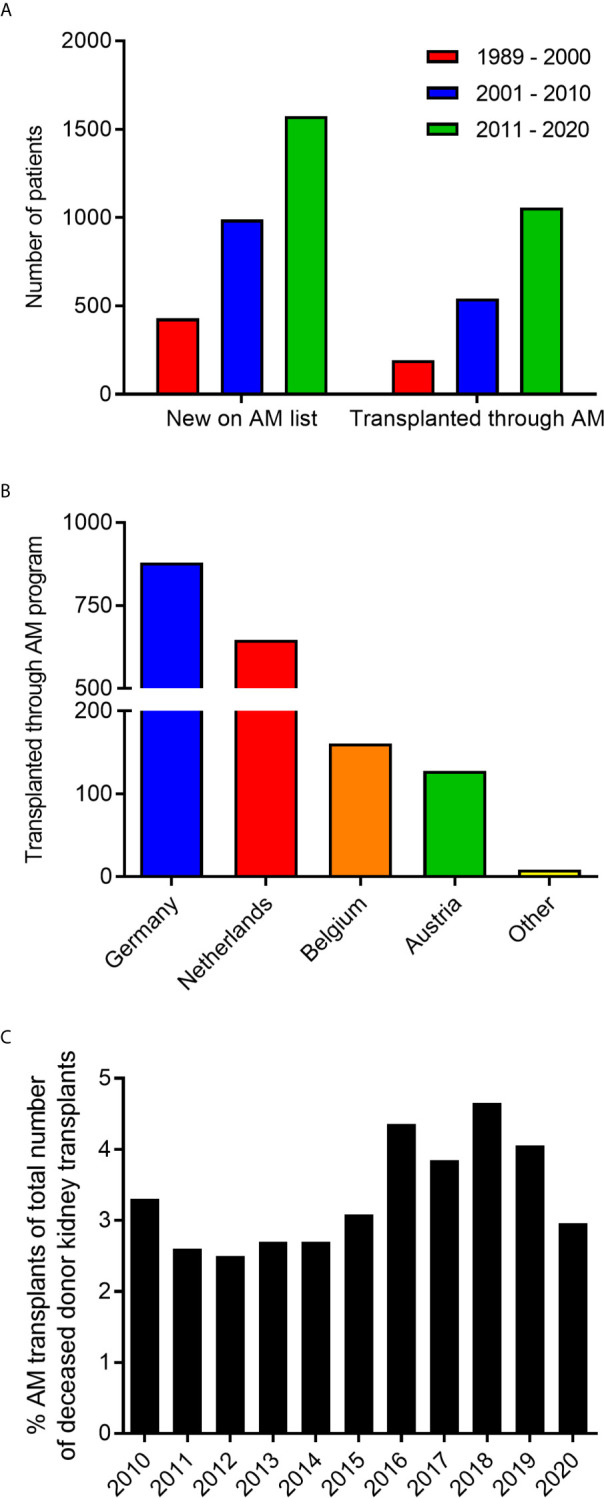
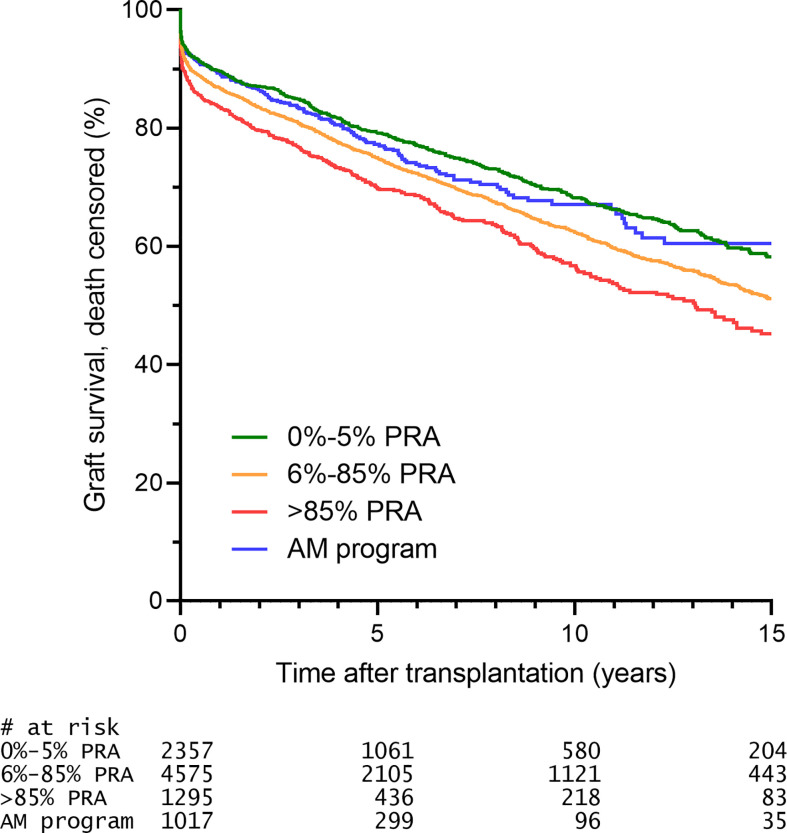
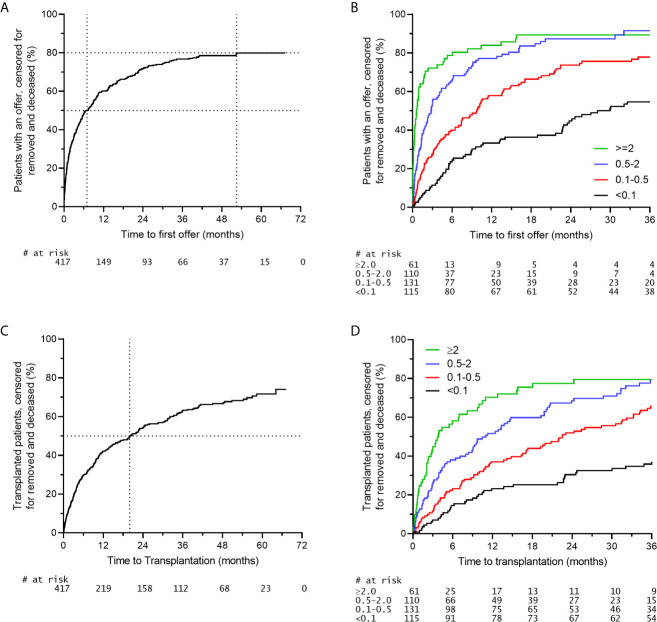
Highly sensitized kidney patients accrue on the transplant waiting list due to their broad immunization against non-self Human Leucocyte Antigens (HLA). Although challenging, the best option for highly sensitized patients is transplantation with a crossmatch negative donor without any additional therapeutic intervention. The Eurotransplant Acceptable Mismatch (AM) program was initiated more than 30 years ago with the intention to increase the chance for highly sensitized patients to be transplanted with such a compatible donor. The AM program allows for enhanced transplantation to this difficult to transplant patient group by allocating deceased donor kidneys on the basis of a match with the recipient's own HLA antigens in combination with predefined acceptable antigens. Acceptable antigens are those HLA antigens towards which the patients has never formed antibodies, as determined by extensive laboratory testing. By using this extended HLA phenotype for allocation and giving priority whenever a compatible donor organ becomes available, organ offers are made for roughly 80% of patients in this program. Up till now, more than 1700 highly sensitized patients have been transplanted through the AM program. Recent studies have shown that the concept of acceptable mismatches being truly immunologically acceptable holds true for both rejection rates and long-term graft survival. Patients that were transplanted through the AM program had a similar rejection incidence and long-term graft survival rates identical to non-sensitized patients transplanted through regular allocation. However, a subset of patients included in the AM program does not receive an organ offer within a reasonable time frame. As these are often patients with a rare HLA phenotype in comparison to the Eurotransplant donor population, extension of the donor pool for these specific patients through further European collaboration would significantly increase their chances of being transplanted. For those patients that will not benefit from such strategy, desensitization is the ultimate solution.
高度致敏的肾脏患者由于广泛针对非自身人类白细胞抗原 (HLA) 的免疫而在移植等待名单上积累。尽管具有挑战性,但高度致敏患者的最佳选择是与交叉配型阴性供体进行移植,而无需任何额外的治疗干预。Eurotransplant 可接受错配 (AM) 计划于 30 多年前启动,旨在增加高度致敏患者与这种相容供体进行移植的机会。该 AM 计划通过根据与受者自身 HLA 抗原的匹配分配已故供体肾脏,并结合预定义的可接受抗原,为这一难以移植的患者群体增强了移植的机会。可接受的抗原是指患者从未形成抗体的 HLA 抗原,这是通过广泛的实验室测试确定的。通过使用这种扩展的 HLA 表型进行分配,并在兼容供体器官可用时给予优先权,该计划中大约 80%的患者会获得器官提供。迄今为止,已有超过 1700 名高度致敏患者通过 AM 计划接受了移植。最近的研究表明,可接受错配在真正的免疫上可接受的概念对排斥率和长期移植物存活率都适用。通过 AM 计划移植的患者的排斥发生率和长期移植物存活率与通过常规分配移植的非致敏患者相似。然而,在 AM 计划中包括的一部分患者在合理的时间内没有获得器官提供。由于这些患者与 Eurotransplant 供体人群相比 HLA 表型较为罕见,因此通过进一步的欧洲合作扩展这些特定患者的供体库将显著增加他们移植的机会。对于那些无法从这种策略中受益的患者,脱敏是最终的解决方案。